Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Jurnal Comentary DirectDocumento3 páginasJurnal Comentary DirectNurul AmaliaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Pathognenesin Immunology, and Diagnosis of Latent M. Tuberculosis InfectionDocumento18 páginasPathognenesin Immunology, and Diagnosis of Latent M. Tuberculosis InfectionNurul AmaliaAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Jurnal RefratDocumento6 páginasJurnal RefratNurul AmaliaAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Resar - AnemiaPathophysiologyEvaluation 07.09.12Documento57 páginasResar - AnemiaPathophysiologyEvaluation 07.09.12addicaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- 1304 FullDocumento8 páginas1304 FullNurul AmaliaAinda não há avaliações
- Jurnal Extrak EtanolDocumento12 páginasJurnal Extrak EtanolAditya Nugie PrasetyoAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
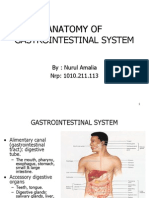
- Anatomi Sistem PencernaanDocumento97 páginasAnatomi Sistem PencernaanNurul AmaliaAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Hypo Glice MiaDocumento13 páginasHypo Glice MiaNurul AmaliaAinda não há avaliações
- AscarisDocumento16 páginasAscarisNurul AmaliaAinda não há avaliações
- AscarisDocumento16 páginasAscarisNurul AmaliaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- PathophysiologyDocumento34 páginasPathophysiologyeunams_1195% (20)
- Congestive Heart FailureDocumento5 páginasCongestive Heart FailureKaren PanganibanAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- CHARM Alt TrialDocumento5 páginasCHARM Alt TrialCristian Villarroel SAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Summer Project 2Documento58 páginasSummer Project 2Dinesh VidhaniAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Essential HypertensionDocumento13 páginasEssential HypertensionIvan KurniadiAinda não há avaliações
- Phase II Block I - Pharmacology Question Paper B & C SectionsDocumento2 páginasPhase II Block I - Pharmacology Question Paper B & C SectionsMayank Singhal100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- حالات سكرDocumento13 páginasحالات سكرNada AliAinda não há avaliações
- Antihypertensive DrugsDocumento28 páginasAntihypertensive DrugsAdinanta Purnawijaya100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Eplerenone (Inspra)Documento13 páginasEplerenone (Inspra)asdwasdAinda não há avaliações
- Congestive Heart Failure ReportDocumento6 páginasCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- Ch-13 Drugs Used in Heart FailureDocumento49 páginasCh-13 Drugs Used in Heart FailureShabrin SadikhAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The List of Abbreviations For Clerking CaseDocumento20 páginasThe List of Abbreviations For Clerking CaseNur Arthirah Raden100% (1)
- Meds Affecting Blood PressureDocumento5 páginasMeds Affecting Blood PressuremikiAinda não há avaliações
- Nephrotic Syndrome-1Documento21 páginasNephrotic Syndrome-1Wondimu EliasAinda não há avaliações
- Guía Rápida StanfordDocumento6 páginasGuía Rápida StanfordDr. Victor Adolfo RochaAinda não há avaliações
- Sop CFLTC 14.06.20Documento55 páginasSop CFLTC 14.06.20madhusoodhananppAinda não há avaliações
- How To Prescribe ENTRESTO To Your Patients: Dosing and Titration GuideDocumento3 páginasHow To Prescribe ENTRESTO To Your Patients: Dosing and Titration GuideCorina DiaconescuAinda não há avaliações
- 1 Drugs For HypertensionDocumento62 páginas1 Drugs For HypertensionSaniAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- IAE-C117-06010-EN - Novartis Un Nuevo Lanzamiento en Latinoamerica - ADocumento20 páginasIAE-C117-06010-EN - Novartis Un Nuevo Lanzamiento en Latinoamerica - AAlan DonosoAinda não há avaliações
- Uci Protocol Brighman BostonDocumento43 páginasUci Protocol Brighman BostonAnonymous ZUaUz1wwAinda não há avaliações
- Algoritma Tatalaksana HTDocumento2 páginasAlgoritma Tatalaksana HTUswatun Hasanah RIAinda não há avaliações
- Anesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) AmidesDocumento3 páginasAnesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) Amidesammar amerAinda não há avaliações
- Nac Osce Comprehensive ReviewDocumento177 páginasNac Osce Comprehensive ReviewAisha SyedAinda não há avaliações
- Effect of Finerenone On Chronic Kidney Disease Outcomes in Type 2 DiabetesDocumento27 páginasEffect of Finerenone On Chronic Kidney Disease Outcomes in Type 2 DiabetesMayi GfAinda não há avaliações
- Oman Prometric Exam NotesDocumento417 páginasOman Prometric Exam NotesMuhammad Amin93% (14)
- Blocker (CCB) Used On Obstructive Sleep Apnea (OSA) Incidence in HypertensionDocumento10 páginasBlocker (CCB) Used On Obstructive Sleep Apnea (OSA) Incidence in HypertensionDhanang Prawira NugrahaAinda não há avaliações
- OB Evals 2Documento32 páginasOB Evals 2Zelle Pamplona RamosAinda não há avaliações
- Acute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihaDocumento98 páginasAcute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihablackcatAinda não há avaliações
- A GLIMPSE Into Cardiology 2022Documento48 páginasA GLIMPSE Into Cardiology 2022Ashvanee Kumar SharmaAinda não há avaliações
- Nature Made HandoutDocumento8 páginasNature Made Handoutr.sorghabiAinda não há avaliações