Você também pode gostar
- Kurt Cobain Case StudyDocumento11 páginasKurt Cobain Case StudyKC Respicio67% (3)
- A Few Online Resources For DBTDocumento6 páginasA Few Online Resources For DBTAnkur SinghAinda não há avaliações
- Mechanisms of Change in DBT for BPDDocumento5 páginasMechanisms of Change in DBT for BPDSarita ValenzuelaAinda não há avaliações
- Unit 9 - Mental HealthDocumento35 páginasUnit 9 - Mental HealthKhushi GillAinda não há avaliações
- Session 26 A NP Conference Handout - Session 5Documento8 páginasSession 26 A NP Conference Handout - Session 5SFLD100% (1)
- Treatment PlanDocumento4 páginasTreatment Planworship himAinda não há avaliações
- Outline of A Case Study ReportDocumento14 páginasOutline of A Case Study ReportdnsgabonAinda não há avaliações
- OCD and Psychological ManagementDocumento35 páginasOCD and Psychological ManagementhelalAinda não há avaliações
- Understanding Your AnxietyDocumento79 páginasUnderstanding Your AnxietyMr. Lira100% (1)
- OcdDocumento15 páginasOcdapi-272821843Ainda não há avaliações
- A Basic Breathing TechniqueDocumento6 páginasA Basic Breathing TechniqueFebbe Nadia Okky LucianaAinda não há avaliações
- MENTAL HEALTH GUIDE YOUTH WORKERSDocumento37 páginasMENTAL HEALTH GUIDE YOUTH WORKERSStacia CunninghamAinda não há avaliações
- 03 Psycheck Clinical TreatmentDocumento147 páginas03 Psycheck Clinical TreatmentJohnny TorresAinda não há avaliações
- MENTAL HEALTH CONCEPT PSYCHOTHERAPEUTIC MODALITIES-mondayDocumento4 páginasMENTAL HEALTH CONCEPT PSYCHOTHERAPEUTIC MODALITIES-mondayDyanne BautistaAinda não há avaliações
- Adjustment DisorderDocumento37 páginasAdjustment DisorderprabhaAinda não há avaliações
- Clinical Guidelines For Improving Dialectical Thinking in DBTDocumento15 páginasClinical Guidelines For Improving Dialectical Thinking in DBTMaria MartinezAinda não há avaliações
- Twenty Questions To Help You Challenge Negative Thoughts: What Is The Evidence?Documento5 páginasTwenty Questions To Help You Challenge Negative Thoughts: What Is The Evidence?Adel OmarAinda não há avaliações
- Everything You Need to Know About Eating Disorder RecoveryDocumento16 páginasEverything You Need to Know About Eating Disorder Recoverynn100% (2)
- Healing Inside Out And Outside In: Finding Zen through Spriritual HealingNo EverandHealing Inside Out And Outside In: Finding Zen through Spriritual HealingAinda não há avaliações
- 57 Psychopathology OCD 2007PDFDocumento4 páginas57 Psychopathology OCD 2007PDFLIDIYA MOL P VAinda não há avaliações
- Clinical Application of The DSM-5 in Private CounselingDocumento15 páginasClinical Application of The DSM-5 in Private CounselingRoss CameronAinda não há avaliações
- Social Anxietyand Cognitive Behavioural TechniquesDocumento14 páginasSocial Anxietyand Cognitive Behavioural TechniquesAlfonso DíezAinda não há avaliações
- BibliographyDocumento146 páginasBibliographyLourdu XavierAinda não há avaliações
- CBTDocumento13 páginasCBTAmit TamboliAinda não há avaliações
- Psychosocialintervention 2Documento172 páginasPsychosocialintervention 2Roh Jiten100% (1)
- Everything Counselors and Supervisors Need To Know About Treating Trauma Bicknell Hentges LynchDocumento14 páginasEverything Counselors and Supervisors Need To Know About Treating Trauma Bicknell Hentges LynchTeri WILSONAinda não há avaliações
- PsychotherapyDocumento47 páginasPsychotherapyanisha batraAinda não há avaliações
- Counselling NotesDocumento925 páginasCounselling Notesrina_singh47796200% (1)
- MindfulnessAsTherapy HuxterDocumento13 páginasMindfulnessAsTherapy Huxterelena.an15Ainda não há avaliações
- Integrative Approaches To Anxiety: Easing The Fear: What Is Anxiety? Causes of AnxietyDocumento7 páginasIntegrative Approaches To Anxiety: Easing The Fear: What Is Anxiety? Causes of AnxietyBojana VulasAinda não há avaliações
- Rather Than Desirable, Outcomes.: What Is Impulsivity?Documento7 páginasRather Than Desirable, Outcomes.: What Is Impulsivity?Suresh LukoseAinda não há avaliações
- Salas Bowen TheoryDocumento32 páginasSalas Bowen TheoryJade Harris ColorjeAinda não há avaliações
- Stress and Its ManagementDocumento31 páginasStress and Its ManagementMelody Shekhar100% (1)
- How To Overcome Fear and Anxiety: What Makes You Afraid?Documento5 páginasHow To Overcome Fear and Anxiety: What Makes You Afraid?Boda Tanvi100% (1)
- Psychiatric Rehabilitation and Recovery ProgramsDocumento10 páginasPsychiatric Rehabilitation and Recovery ProgramsSunil Shekhar NayakAinda não há avaliações
- Fundamentals To Clinical PsychologyDocumento6 páginasFundamentals To Clinical PsychologySurabhi RanjanAinda não há avaliações
- Case Analysis: Bipolar 1 Diagnosis & Treatment PlanDocumento2 páginasCase Analysis: Bipolar 1 Diagnosis & Treatment PlanJoshua Ringor100% (1)
- Cognitive Behavior TherapyDocumento8 páginasCognitive Behavior TherapyKerem Ali YavuzAinda não há avaliações
- Motivational Therapy (Or MT) Is A Combination ofDocumento2 páginasMotivational Therapy (Or MT) Is A Combination ofRumana AliAinda não há avaliações
- Acute Distress Tolerance SkillsDocumento8 páginasAcute Distress Tolerance SkillsEgylany Lany100% (1)
- Nursing Care Plan: Coughing or Gagging When Swallowing Having To Cut Food Into Smaller Pieces orDocumento5 páginasNursing Care Plan: Coughing or Gagging When Swallowing Having To Cut Food Into Smaller Pieces orMaria CabangonAinda não há avaliações
- MCQ on Types of GlomerulonephritisDocumento3 páginasMCQ on Types of GlomerulonephritisIM CT50% (2)
- Delusional DisorderDocumento4 páginasDelusional DisorderBarunansu SarkarAinda não há avaliações
- OCD: Obsessions, Compulsions, TreatmentsDocumento23 páginasOCD: Obsessions, Compulsions, TreatmentsSónia AlvesAinda não há avaliações
- What's NextDocumento27 páginasWhat's NextBethany House PublishersAinda não há avaliações
- RCPsych Leaflet On CBTDocumento7 páginasRCPsych Leaflet On CBTZee YongAinda não há avaliações
- Psychology of Stress Module 1Documento75 páginasPsychology of Stress Module 1NIDA MPAinda não há avaliações
- What Are Anxiety Disorders?Documento2 páginasWhat Are Anxiety Disorders?Corina MihaelaAinda não há avaliações
- Clinical Social Work: Privilege FormDocumento1 páginaClinical Social Work: Privilege FormjirehcounselingAinda não há avaliações
- Chapter 5 AnxietyDocumento16 páginasChapter 5 AnxietyMark Jayson JuevesAinda não há avaliações
- Stress and Anxiety For College Student3Documento10 páginasStress and Anxiety For College Student3sheri alexanderAinda não há avaliações
- Theories of CounselingDocumento10 páginasTheories of Counselingབཀྲཤིས ཚེརིངAinda não há avaliações
- Causes and Types of DementiaDocumento9 páginasCauses and Types of DementiaAmrita DeAinda não há avaliações
- Anxiety DisorderDocumento11 páginasAnxiety Disordermzunl25476Ainda não há avaliações
- Suicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideDocumento12 páginasSuicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideShreeya GhagAinda não há avaliações
- Obsessive Compulsive DisorderDocumento45 páginasObsessive Compulsive DisorderPriya Darishini GunasegaranAinda não há avaliações
- Mental Status Exam TemplateDocumento2 páginasMental Status Exam TemplateNicholasAinda não há avaliações
- Ncmhce Sample Case StudiesDocumento6 páginasNcmhce Sample Case Studies002019ryAinda não há avaliações
- Be Confident Come Out of Your Shell at Work and PlayDocumento25 páginasBe Confident Come Out of Your Shell at Work and PlayKeep Left Sopa0% (1)
- Exploring Suicidal BehaviorDocumento5 páginasExploring Suicidal BehaviorMatt KunAinda não há avaliações
- SFP EasyIntroToEganDocumento5 páginasSFP EasyIntroToEganAlbert Muya MurayaAinda não há avaliações
- NIMH4 S DBT Diary Cards With InstructionsDocumento4 páginasNIMH4 S DBT Diary Cards With Instructionsmary grace bana100% (1)
- Safe SexDocumento11 páginasSafe SexnathanAinda não há avaliações
- Route To: Nnovative Joints Ejuvenation CentreDocumento2 páginasRoute To: Nnovative Joints Ejuvenation CentreAnil Kumar.VAinda não há avaliações
- Anterior Segment OctDocumento53 páginasAnterior Segment OctA.c. RaghuAinda não há avaliações
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamDocumento21 páginasChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoAinda não há avaliações
- Uncorrected Author ProofDocumento15 páginasUncorrected Author ProofindahAinda não há avaliações
- Prescriptions On Asthma & APDDocumento9 páginasPrescriptions On Asthma & APDeesha shahAinda não há avaliações
- Medical Handwashing Procedure StepsDocumento3 páginasMedical Handwashing Procedure StepsKERL RAMAAinda não há avaliações
- C-Section Guide: What to Expect with Cesarean DeliveryDocumento3 páginasC-Section Guide: What to Expect with Cesarean DeliveryFEALABREPORTSAinda não há avaliações
- 42fundus AngiographyDocumento28 páginas42fundus AngiographyHitesh SharmaAinda não há avaliações
- Effect of Temperature On FrogDocumento2 páginasEffect of Temperature On FrogPrerna DubeyAinda não há avaliações
- Vancouver Coastal Health Enhanced Surveillance and Precautions ProtocolsDocumento1 páginaVancouver Coastal Health Enhanced Surveillance and Precautions ProtocolsIan YoungAinda não há avaliações
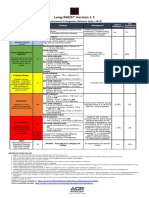
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Documento1 páginaLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotAinda não há avaliações
- Amavatha & VathasonithaDocumento125 páginasAmavatha & VathasonithaCicil AbrahamAinda não há avaliações
- Milobar Alexus Resume MayoDocumento2 páginasMilobar Alexus Resume Mayoapi-338646789Ainda não há avaliações
- Type2 Diabetes HandoutDocumento1 páginaType2 Diabetes Handouthendra_darmawan_4Ainda não há avaliações
- Urolithiasis Overview: Classification, Pathogenesis and Treatment ModalitiesDocumento38 páginasUrolithiasis Overview: Classification, Pathogenesis and Treatment Modalitiesraed ganmAinda não há avaliações
- Important Classifications PDFDocumento42 páginasImportant Classifications PDF330 Himank MehtaAinda não há avaliações
- Complications of 3rd TrimesterDocumento49 páginasComplications of 3rd TrimesterMA. JYRELL BONITOAinda não há avaliações
- Retrograde Intubation Using Epidural Catheter - A Safe and Cost Effective Technique - A Case ReportDocumento2 páginasRetrograde Intubation Using Epidural Catheter - A Safe and Cost Effective Technique - A Case ReportIOSRjournalAinda não há avaliações
- Lesson 1Documento20 páginasLesson 1Irish Jean AgsawayAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar PustakaNurfauziyahAinda não há avaliações
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDocumento21 páginasMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89Ainda não há avaliações
- Case Report模板Documento18 páginasCase Report模板ChenAinda não há avaliações
- Basic pharmacology of anaesthesia drugs in 40 charactersDocumento56 páginasBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87Ainda não há avaliações
- Conscious Sedation PaediatricsDocumento44 páginasConscious Sedation PaediatricsReeta TaxakAinda não há avaliações
- Optima GutDocumento11 páginasOptima GutNoly ClaveringAinda não há avaliações
- Nursing Management - Colon CancerDocumento7 páginasNursing Management - Colon CancerReese Alessandra GandulfoAinda não há avaliações