Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Guidance for Processing SushiDocumento24 páginasGuidance for Processing SushigsyaoAinda não há avaliações
- Knowledge and Perception of Selected High School Students With Regards To Sex Education and Its ContentDocumento4 páginasKnowledge and Perception of Selected High School Students With Regards To Sex Education and Its ContentJeffren P. Miguel0% (1)
- STSDSD QuestionDocumento12 páginasSTSDSD QuestionAakash DasAinda não há avaliações
- Community Tax Certificate PRINTDocumento2 páginasCommunity Tax Certificate PRINTClarenz0% (1)
- Exam 2 Study GuideDocumento11 páginasExam 2 Study GuideAnonymous ewJy7jyvNAinda não há avaliações
- Anti Viral DrugsDocumento6 páginasAnti Viral DrugskakuAinda não há avaliações
- Alice Corporation Pty. Ltd. v. CLS Bank International and CLS Services Ltd.Documento4 páginasAlice Corporation Pty. Ltd. v. CLS Bank International and CLS Services Ltd.Rachel PauloseAinda não há avaliações
- (AC-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz - INGLES III (14653)Documento3 páginas(AC-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz - INGLES III (14653)Eduardo Arucutipa60% (5)
- Efecto de at en Grupos para La SaludDocumento5 páginasEfecto de at en Grupos para La SaludpsychforallAinda não há avaliações
- Deterioro Neuropsicológico en Esquizofrenia Desde El Periodo Premórbido Al Inicio de La EnfermedadDocumento11 páginasDeterioro Neuropsicológico en Esquizofrenia Desde El Periodo Premórbido Al Inicio de La EnfermedadpsychforallAinda não há avaliações
- The Lancent Cognitive Therapy For People With Schizophrenia Spectrum Disorders Not Taking Antipsychotic Drugs. A Single Blind Randomised Controlled Trial 2014Documento9 páginasThe Lancent Cognitive Therapy For People With Schizophrenia Spectrum Disorders Not Taking Antipsychotic Drugs. A Single Blind Randomised Controlled Trial 2014sharp8787Ainda não há avaliações
- Globalising Mental Health: A Neoliberal ProjectDocumento7 páginasGlobalising Mental Health: A Neoliberal ProjectlizardocdAinda não há avaliações
- Diagnóstico Psiquiátrico Como Instrumento PolíticoDocumento13 páginasDiagnóstico Psiquiátrico Como Instrumento PolíticopsychforallAinda não há avaliações
- Personalidad y Respuesta Al TerapeutaDocumento7 páginasPersonalidad y Respuesta Al TerapeutapsychforallAinda não há avaliações
- Plasticidad Cerebral Inducida Por ECT Determina Beneficios en Trastornos AfectivosDocumento6 páginasPlasticidad Cerebral Inducida Por ECT Determina Beneficios en Trastornos AfectivospsychforallAinda não há avaliações
- Perfeccionamiento de Las Técnicas de ECTDocumento15 páginasPerfeccionamiento de Las Técnicas de ECTpsychforallAinda não há avaliações
- The Network of Global Corporate ControlDocumento36 páginasThe Network of Global Corporate ControlpsychforallAinda não há avaliações
- Forum World Psychiatry No Adherencia A La Medicación en Personas Con Psicosis - Oct 2013Documento24 páginasForum World Psychiatry No Adherencia A La Medicación en Personas Con Psicosis - Oct 2013psychforallAinda não há avaliações
- Médicos Bajo La Influencia de La Industria FarmacéuticaDocumento27 páginasMédicos Bajo La Influencia de La Industria FarmacéuticapsychforallAinda não há avaliações
- Efectos de La Música en La Reducción de Ansiedad en Personas en UCIDocumento10 páginasEfectos de La Música en La Reducción de Ansiedad en Personas en UCIpsychforallAinda não há avaliações
- World Health Day 2013Documento64 páginasWorld Health Day 2013koromakAinda não há avaliações
- El Mito de La Esquizofrenia Como Enfermedad Cerebral ProgresivaDocumento10 páginasEl Mito de La Esquizofrenia Como Enfermedad Cerebral ProgresivapsychforallAinda não há avaliações
- Mortalidad en Anorexia y Bulimia NerviosaDocumento9 páginasMortalidad en Anorexia y Bulimia NerviosapsychforallAinda não há avaliações
- Current Rapid Tranquillisation Documents in The UKDocumento9 páginasCurrent Rapid Tranquillisation Documents in The UKpsychforallAinda não há avaliações
- Suicidio Entre Soldados - Factores de Riesgo y ProtecciónDocumento29 páginasSuicidio Entre Soldados - Factores de Riesgo y ProtecciónpsychforallAinda não há avaliações
- Amphetamine - Past and PresentDocumento18 páginasAmphetamine - Past and Presentpsychforall100% (1)
- Disfunción Cerebral Del DesarrolloDocumento9 páginasDisfunción Cerebral Del DesarrollopsychforallAinda não há avaliações
- A Survey of The Use of Emergency Parenteral Medication at A Secure Psychiatric HospitalDocumento8 páginasA Survey of The Use of Emergency Parenteral Medication at A Secure Psychiatric HospitalpsychforallAinda não há avaliações
- Medical Guidelines For PICU Seclusion ReviewsDocumento11 páginasMedical Guidelines For PICU Seclusion ReviewspsychforallAinda não há avaliações
- Identification of Risk Loci With Shared Effects On Five Major Psychiatric Disorders: A Genome-Wide Analysis - The Lancet 28. Feb 2013Documento9 páginasIdentification of Risk Loci With Shared Effects On Five Major Psychiatric Disorders: A Genome-Wide Analysis - The Lancet 28. Feb 2013oxidizedsoulAinda não há avaliações
- Tipología de Personas Con TMGDocumento10 páginasTipología de Personas Con TMGpsychforallAinda não há avaliações
- Cytochrome P450-Mediated Drug Metabolism in The BrainDocumento12 páginasCytochrome P450-Mediated Drug Metabolism in The BrainpsychforallAinda não há avaliações
- Tasers and PsychiatryDocumento7 páginasTasers and PsychiatrypsychforallAinda não há avaliações
- The Role of Serotonin in Cognitive FunctionDocumento10 páginasThe Role of Serotonin in Cognitive FunctionpsychforallAinda não há avaliações
- Enigmática Persistencia de La Anorexia NerviosaDocumento8 páginasEnigmática Persistencia de La Anorexia NerviosapsychforallAinda não há avaliações
- Relaciones Sociales y Riesgo de MortalidadDocumento20 páginasRelaciones Sociales y Riesgo de MortalidadpsychforallAinda não há avaliações
- Psicosis Secundaria - Actualización 2013Documento12 páginasPsicosis Secundaria - Actualización 2013psychforallAinda não há avaliações
- Aspectos Psicológicos y Neurobiológicos Del Estrés y Su Relevancia en El Entrenamiento de Médicos ResidentesDocumento5 páginasAspectos Psicológicos y Neurobiológicos Del Estrés y Su Relevancia en El Entrenamiento de Médicos ResidentespsychforallAinda não há avaliações
- Economics 1A and B WorkbookDocumento90 páginasEconomics 1A and B WorkbookmrlsrpssqbucxwswfjAinda não há avaliações
- Shah Wali Ullah Syed Haji Shariat Ullah Ahmad Barelvi (Notes)Documento2 páginasShah Wali Ullah Syed Haji Shariat Ullah Ahmad Barelvi (Notes)Samreen KapasiAinda não há avaliações
- Biological Control in Brazil An OverviewDocumento10 páginasBiological Control in Brazil An OverviewGustavo Ferreira MoraisAinda não há avaliações
- Pirate+Borg BeccaDocumento1 páginaPirate+Borg BeccaamamAinda não há avaliações
- Lincoln's Last Trial by Dan AbramsDocumento6 páginasLincoln's Last Trial by Dan AbramsdosatoliAinda não há avaliações
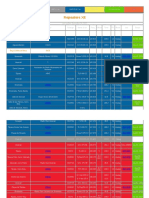
- Repeaters XE PDFDocumento12 páginasRepeaters XE PDFenzzo molinariAinda não há avaliações
- Gautam KDocumento12 páginasGautam Kgautam kayapakAinda não há avaliações
- IDocumento8 páginasICarlaSampaioAinda não há avaliações
- Affidavit of Loss Drivers License AffidavitDocumento2 páginasAffidavit of Loss Drivers License AffidavitJov May Dimco50% (2)
- Samonte Vs CADocumento7 páginasSamonte Vs CAMaricel Caranto FriasAinda não há avaliações
- Inmarsat M2M Terminal ComparisonDocumento2 páginasInmarsat M2M Terminal Comparisonmaruka33Ainda não há avaliações
- 3D Model of Steam Engine Using Opengl: Indian Institute of Information Technology, AllahabadDocumento18 páginas3D Model of Steam Engine Using Opengl: Indian Institute of Information Technology, AllahabadRAJ JAISWALAinda não há avaliações
- Who Is Marine Le PenDocumento6 páginasWho Is Marine Le PenYusuf Ali RubelAinda não há avaliações
- Senior SAP Engineer ResumeDocumento1 páginaSenior SAP Engineer ResumeSatish Acharya NamballaAinda não há avaliações
- Sach Bai Tap Tieng Anh8 - Mai Lan HuongDocumento157 páginasSach Bai Tap Tieng Anh8 - Mai Lan Huongvothithao19750% (1)
- Describing A CompanyDocumento3 páginasDescribing A CompanyAfnanAinda não há avaliações
- BiOWiSH Crop OverviewDocumento2 páginasBiOWiSH Crop OverviewBrian MassaAinda não há avaliações
- The Names & Atributes of Allah - Abdulillah LahmamiDocumento65 páginasThe Names & Atributes of Allah - Abdulillah LahmamiPanthera_Ainda não há avaliações
- Wa0004.Documento85 páginasWa0004.sheetalsri1407Ainda não há avaliações
- Focus2 2E Review Test 4 Units1 8 Vocabulary Grammar UoE Reading GroupBDocumento4 páginasFocus2 2E Review Test 4 Units1 8 Vocabulary Grammar UoE Reading GroupBaides1sonAinda não há avaliações
- Urbanization As A Transformative Force: Quick FactsDocumento20 páginasUrbanization As A Transformative Force: Quick FactsJulio CovarrubiasAinda não há avaliações
- Official Correspondence in English CompleteDocumento55 páginasOfficial Correspondence in English Completeyadab rautAinda não há avaliações