Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Aging Brain: Course GuidebookDocumento126 páginasThe Aging Brain: Course GuidebookIsabel Cristina Jaramillo100% (2)
- A656 GR 80 Brochure 06-26-08Documento2 páginasA656 GR 80 Brochure 06-26-08OsmanAinda não há avaliações
- Material Rate PWD 2014...........Documento70 páginasMaterial Rate PWD 2014...........Shamsul IslamAinda não há avaliações
- EESC 111 Worksheets Module 5Documento5 páginasEESC 111 Worksheets Module 5Keira O'HowAinda não há avaliações
- Plastic As Soil StabilizerDocumento28 páginasPlastic As Soil StabilizerKhald Adel KhaldAinda não há avaliações
- Unit Two The Health Benefits of Physical ActivityDocumento10 páginasUnit Two The Health Benefits of Physical ActivityYoseph DefaruAinda não há avaliações
- 8953-Specifications For Doosan Man 9l21 31Documento7 páginas8953-Specifications For Doosan Man 9l21 31Bae Juyeon100% (1)
- CAT Test Series - 2014Documento2 páginasCAT Test Series - 2014dimevsnAinda não há avaliações
- Jurnal Gerd PDFDocumento6 páginasJurnal Gerd PDFdilaAinda não há avaliações
- Hotel Elizabeth in Baguio City: Address: J Felipe Street Cor. Gibraltar Road Mines View Park, Baguio City, PhilippinesDocumento16 páginasHotel Elizabeth in Baguio City: Address: J Felipe Street Cor. Gibraltar Road Mines View Park, Baguio City, PhilippinesI amEllaAinda não há avaliações
- Pamela Johnson Arnold and Nancy Fortson On Behalf of A Minor Vs Hamilton Co. Dept. of EducationDocumento27 páginasPamela Johnson Arnold and Nancy Fortson On Behalf of A Minor Vs Hamilton Co. Dept. of EducationDan LehrAinda não há avaliações
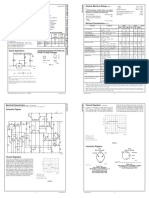
- LM 337Documento4 páginasLM 337matias robertAinda não há avaliações
- 1979 The Cult Phenomenon in The United States - DR John Gordon ClarkDocumento8 páginas1979 The Cult Phenomenon in The United States - DR John Gordon ClarkFrederick BismarkAinda não há avaliações
- MGMTDocumento19 páginasMGMTMakrant MohanAinda não há avaliações
- PL00002949Documento5 páginasPL00002949Nino AlicAinda não há avaliações
- Dual Laminate Piping HandbookDocumento46 páginasDual Laminate Piping HandbookA.Subin DasAinda não há avaliações
- The Development of Attachment in Separated and Divorced FamiliesDocumento33 páginasThe Development of Attachment in Separated and Divorced FamiliesInigo BorromeoAinda não há avaliações
- MINUZA Laptop Scheme Programs ThyDocumento9 páginasMINUZA Laptop Scheme Programs Thyanualithe kamalizaAinda não há avaliações
- ReferensiDocumento4 páginasReferensiyusri polimengoAinda não há avaliações
- An Enhanced Model of Thermo Mechanical Loading On A Vaccum Insulated GlazingDocumento29 páginasAn Enhanced Model of Thermo Mechanical Loading On A Vaccum Insulated GlazingNguyễn SơnAinda não há avaliações
- PMA 2015 2016 Issue 3 PDFDocumento36 páginasPMA 2015 2016 Issue 3 PDFLyndon Mercado TolentinoAinda não há avaliações
- Written Assignment Unit 4 Health ScienceDocumento6 páginasWritten Assignment Unit 4 Health SciencesafsdaAinda não há avaliações
- NASA ISS Expedition 2 Press KitDocumento27 páginasNASA ISS Expedition 2 Press KitOrion2015Ainda não há avaliações
- BRS PDFDocumento14 páginasBRS PDFGautam KhanwaniAinda não há avaliações
- Governance StructureDocumento1 páginaGovernance StructureJoydip MukhopadhyayAinda não há avaliações
- HSN-Lube 2007 PDFDocumento45 páginasHSN-Lube 2007 PDFCecilio Valderrama100% (3)
- ISCO HDPE Full Line CatalogDocumento252 páginasISCO HDPE Full Line Catalogpvsreddy2002100% (1)
- House of Candy PresentationDocumento42 páginasHouse of Candy PresentationRohit JaroudiyaAinda não há avaliações
- Microbes in Human Welfare PDFDocumento2 páginasMicrobes in Human Welfare PDFshodhan shettyAinda não há avaliações
- Decision Making in Perioperative Medicine Clinical Pearls 2021Documento351 páginasDecision Making in Perioperative Medicine Clinical Pearls 2021Dal RdzAinda não há avaliações