Você também pode gostar
- Herpes Zoster in The Pediatric Age Group: Study From A Tertiary Care HospitalDocumento4 páginasHerpes Zoster in The Pediatric Age Group: Study From A Tertiary Care HospitalwilandayuAinda não há avaliações
- MR Surya WilandaDocumento6 páginasMR Surya WilandawilandayuAinda não há avaliações
- Pathophysiology: Anemia Thrombocytopenia NeutropeniaDocumento1 páginaPathophysiology: Anemia Thrombocytopenia NeutropeniawilandayuAinda não há avaliações
- Imaging AppendicitisDocumento75 páginasImaging AppendicitiswilandayuAinda não há avaliações
- Aria Rhinitis Allergic Pocket GuideDocumento8 páginasAria Rhinitis Allergic Pocket GuideAlfani FajarAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Bojar PediatricDocumento123 páginasBojar PediatricLuqman AlwiAinda não há avaliações
- Care Plan Unstable AnginaDocumento4 páginasCare Plan Unstable Anginaالغزال الذهبي50% (6)
- IM HandbookaDocumento378 páginasIM HandbookakkAinda não há avaliações
- EkgDocumento75 páginasEkgRamot Tribaya Recardo PardedeAinda não há avaliações
- SVT and DengueDocumento4 páginasSVT and Denguefrengki prasAinda não há avaliações
- Arrhythmias - Cardiovascular Medicine - MKSAP 17Documento17 páginasArrhythmias - Cardiovascular Medicine - MKSAP 17alaaAinda não há avaliações
- Emp SyncopeDocumento20 páginasEmp SyncopeWilmer JimenezAinda não há avaliações
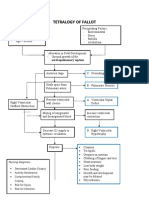
- Concept Map Tetralogy of FallotDocumento2 páginasConcept Map Tetralogy of FallotKarl KiwisAinda não há avaliações
- Defibrillation ChecklistDocumento4 páginasDefibrillation ChecklistCzarina100% (1)
- Ventricular Fibrillation NCPDocumento3 páginasVentricular Fibrillation NCPAjay SupanAinda não há avaliações
- pEDIATRICS Cvs MCQDocumento3 páginaspEDIATRICS Cvs MCQcataztropher88% (8)
- Underground Clinical Vignettes - Pathophysiology I PDFDocumento124 páginasUnderground Clinical Vignettes - Pathophysiology I PDFtwinkle000100% (2)
- Path-09 CARDIODocumento18 páginasPath-09 CARDIOCarlos Fernando Banegas FloresAinda não há avaliações
- Guidelines For The Interpretation of The Neonatal ElectrocardiogramDocumento16 páginasGuidelines For The Interpretation of The Neonatal ElectrocardiogramccAinda não há avaliações
- The Cox-Maze IV Procedure For Lone Atrial Fibrillation - A Single Center Experience in 100 Consecutive Patients.Documento2 páginasThe Cox-Maze IV Procedure For Lone Atrial Fibrillation - A Single Center Experience in 100 Consecutive Patients.Juan Diego RestrepoAinda não há avaliações
- 2018 ESC-EACTS Guidelines On Myocardial RevascularizationDocumento96 páginas2018 ESC-EACTS Guidelines On Myocardial RevascularizationTony Miguel Saba SabaAinda não há avaliações
- Acute Coronary Syndromes Acute Coronary Syndromes OverviewDocumento8 páginasAcute Coronary Syndromes Acute Coronary Syndromes Overviewمحمد زينAinda não há avaliações
- Dr.C.N.manjunath The Eminent CardiologistDocumento19 páginasDr.C.N.manjunath The Eminent Cardiologistacharla5549100% (1)
- Cardiorespiratory ArrestDocumento5 páginasCardiorespiratory Arrestore wa IzzampAinda não há avaliações
- ACLS Pretest Questions and Answers 2020 (Full Practice Test)Documento23 páginasACLS Pretest Questions and Answers 2020 (Full Practice Test)김민길50% (4)
- Kardiovaskular: Departemen Patologi Anatomi Fakultas Kedokteran Universitas Pembangunan Nasional Jakarta 2012Documento37 páginasKardiovaskular: Departemen Patologi Anatomi Fakultas Kedokteran Universitas Pembangunan Nasional Jakarta 2012Angga AhadiyatAinda não há avaliações
- PacemakerDocumento24 páginasPacemakerLAWKUSH KUMARAinda não há avaliações
- College of Nursing: Pharmacological ManagementDocumento4 páginasCollege of Nursing: Pharmacological ManagementBianca Mikaela DosdosAinda não há avaliações
- Cardiac Catheterization and Coronary Intervention (2nd Edition, 2020)Documento353 páginasCardiac Catheterization and Coronary Intervention (2nd Edition, 2020)John Cancel50% (2)
- Av BlockDocumento38 páginasAv BlockLanna Harumiya100% (1)
- CONCEPT - QuestionsDocumento2 páginasCONCEPT - Questionsgreen_archerAinda não há avaliações
- Lra 181458 Non Operating Room Anesthesia Patient Selection and SpecialDocumento9 páginasLra 181458 Non Operating Room Anesthesia Patient Selection and SpecialEric Aguilar SantiagoAinda não há avaliações
- PMR Poster TBI Takotsubo AAP 2010 PosterDocumento1 páginaPMR Poster TBI Takotsubo AAP 2010 PosterjuanvelasquezAinda não há avaliações
- Case Report VTDocumento12 páginasCase Report VTAnonymous ZbhBxeEVAinda não há avaliações
- Rosuvastatin, Aspirin and ClopidofrelDocumento10 páginasRosuvastatin, Aspirin and ClopidofrelNandan GuptaAinda não há avaliações