Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Land Based SensorsDocumento40 páginasLand Based SensorsJ.MichaelLooneyAinda não há avaliações
- Percentage Conversion Worksheet PDFDocumento2 páginasPercentage Conversion Worksheet PDFJamie LeeAinda não há avaliações
- CO2 Production PlantsDocumento4 páginasCO2 Production PlantsBoojie Recto100% (1)
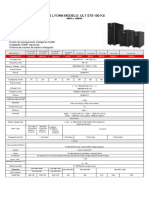
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADocumento1 páginaUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzAinda não há avaliações
- Zebralette User GuideDocumento24 páginasZebralette User GuideGiacomo TimbrelloAinda não há avaliações
- Hydraulic Filter ReportDocumento6 páginasHydraulic Filter ReportSandrock_01sr2Ainda não há avaliações
- VDVDVXVCFDBCVCDocumento390 páginasVDVDVXVCFDBCVCHafiz Rahmat UllahAinda não há avaliações
- AminesDocumento12 páginasAminesEmelda BanumathyAinda não há avaliações
- GH Chap 78 - Insulin, Glucagon and DMDocumento16 páginasGH Chap 78 - Insulin, Glucagon and DMShellz2428Ainda não há avaliações
- Retaining Wall ReporterDocumento18 páginasRetaining Wall ReporterJoefel BessatAinda não há avaliações
- Shop Exercise 5Documento16 páginasShop Exercise 5Athena GrotesqueAinda não há avaliações
- (Altium Tutorial) PCB Symbol Naming ConventionDocumento7 páginas(Altium Tutorial) PCB Symbol Naming ConventionDefne AktemizAinda não há avaliações
- Evaluasi Mutu Fisik, Total Bakteri, Dan Sensori Minuman Sari Tempe Dengan Penambahan Bunga KecombrangDocumento12 páginasEvaluasi Mutu Fisik, Total Bakteri, Dan Sensori Minuman Sari Tempe Dengan Penambahan Bunga KecombrangJosua PakpahanAinda não há avaliações
- Mid-Term Engr 6201 2020Documento3 páginasMid-Term Engr 6201 2020Naseri ShaunAinda não há avaliações
- CS610 Final Term Past Papers Mega FileDocumento35 páginasCS610 Final Term Past Papers Mega Filehowtoplaygames38Ainda não há avaliações
- A B C D Supply I1 1 2 3 4 Deman D I1Documento7 páginasA B C D Supply I1 1 2 3 4 Deman D I1Shaurya DewanAinda não há avaliações
- Matrix Assisted Laser Desorption Ionization Mass Spectrometry Maldi-Tof MsDocumento4 páginasMatrix Assisted Laser Desorption Ionization Mass Spectrometry Maldi-Tof MsElizabeth Katherine Aigaje EspinosaAinda não há avaliações
- Fiber Optics Unit 3Documento82 páginasFiber Optics Unit 3NIKHIL SOLOMON P URK19CS1045Ainda não há avaliações
- Financial Modelling Assignment - Ghizal Naqvi (Attock Petroleum Limited)Documento13 páginasFinancial Modelling Assignment - Ghizal Naqvi (Attock Petroleum Limited)Ghizal NaqviAinda não há avaliações
- 626178a42e9a0 Visual Programming Final PaperDocumento8 páginas626178a42e9a0 Visual Programming Final PaperSaim AhmedAinda não há avaliações
- ZIEHL ABEGG Main Catalogue Centrifugal Fans With IEC Standard MotoDocumento285 páginasZIEHL ABEGG Main Catalogue Centrifugal Fans With IEC Standard MotoTomislav BrezicAinda não há avaliações
- Module 3 - Data and Database ManagementDocumento11 páginasModule 3 - Data and Database ManagementDarrilyn VillalunaAinda não há avaliações
- Test Automation Design PrinciplesDocumento15 páginasTest Automation Design PrinciplesSujay KumarAinda não há avaliações
- Wiring Diagram SCH17: Service InformationDocumento16 páginasWiring Diagram SCH17: Service Informationابو حمزة صبريAinda não há avaliações
- Analyze Sales Performance with Key FiguresDocumento192 páginasAnalyze Sales Performance with Key Figurespanirbanonline3426Ainda não há avaliações
- Manual X-C EFC Diversey Namthip - ENDocumento37 páginasManual X-C EFC Diversey Namthip - ENthouche007Ainda não há avaliações
- Mos PDFDocumento194 páginasMos PDFChoon Ewe LimAinda não há avaliações
- S4M Service ManualDocumento522 páginasS4M Service ManualRafał Krzysztof Kowalski100% (1)
- Project PBLDocumento19 páginasProject PBLAdam LuqmanAinda não há avaliações
- Lab Manual Human PhysiologyDocumento84 páginasLab Manual Human Physiologyaurelya nicoleAinda não há avaliações