Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Renal Stones A Clinical Review PDFDocumento6 páginasRenal Stones A Clinical Review PDFNurholis MajidAinda não há avaliações
- Renal Stones A Clinical Review PDFDocumento6 páginasRenal Stones A Clinical Review PDFNurholis MajidAinda não há avaliações
- External Ear Canal Cholesteatoma and Keratosis Obturans 20070328Documento8 páginasExternal Ear Canal Cholesteatoma and Keratosis Obturans 20070328Nurholis MajidAinda não há avaliações
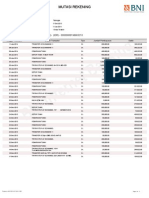
- Mutasi Rekening: Kriteria PencarianDocumento2 páginasMutasi Rekening: Kriteria PencarianNurholis MajidAinda não há avaliações
- Pengaruh Konseling Terhadap Pengetahuan, Sikap, Dan Tindakan Ibu Hamil Tentang Upaya Pencegahan Anemia Masa Kehamilan Di BPS Wilayah Mojo SurabayaDocumento1 páginaPengaruh Konseling Terhadap Pengetahuan, Sikap, Dan Tindakan Ibu Hamil Tentang Upaya Pencegahan Anemia Masa Kehamilan Di BPS Wilayah Mojo SurabayaNurholis MajidAinda não há avaliações
- Bagian Akhir Food RecallDocumento4 páginasBagian Akhir Food RecallNurholis MajidAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Taylor 2018Documento16 páginasTaylor 2018Zahra Alpi SyafilaAinda não há avaliações
- Lumbar DiscopathyDocumento3 páginasLumbar DiscopathyPirasan Traditional Medicine CenterAinda não há avaliações
- Inner SmileDocumento1 páginaInner SmileIon ConstantinAinda não há avaliações
- Case Presentation and Literature Review of Adrenal MassesDocumento50 páginasCase Presentation and Literature Review of Adrenal MassesAnas Mk HindawiAinda não há avaliações
- 191 Biceps Tenodesis RCR V2Documento4 páginas191 Biceps Tenodesis RCR V2mustakAinda não há avaliações
- An Atlas of Surgical AnatomyDocumento246 páginasAn Atlas of Surgical Anatomyartem romanovAinda não há avaliações
- Panfacial Bone Fracture and Medial To Lateral ApproachDocumento20 páginasPanfacial Bone Fracture and Medial To Lateral ApproachDR NASIMAinda não há avaliações
- Jurnal Probo Kak Risna - Id.enDocumento14 páginasJurnal Probo Kak Risna - Id.enaccangAinda não há avaliações
- Anatomy of The Respiratory System: Dersi Sayfa Sayfa Türkçe Dinleyin!Documento9 páginasAnatomy of The Respiratory System: Dersi Sayfa Sayfa Türkçe Dinleyin!fsdgAinda não há avaliações
- Otitis Media With EffusionDocumento3 páginasOtitis Media With EffusionAnish RajAinda não há avaliações
- Guidelines For Basic Adult Neurological Observation: Neurosurgical Nurse Educator NetworkDocumento20 páginasGuidelines For Basic Adult Neurological Observation: Neurosurgical Nurse Educator NetworkSimon S. KledenAinda não há avaliações
- Human Sectional Anatomy Atlas of Body Sections, CT and MRI Images 4ed-127-201Documento75 páginasHuman Sectional Anatomy Atlas of Body Sections, CT and MRI Images 4ed-127-201Elei GiAinda não há avaliações
- Diagnosis of ImpactionDocumento33 páginasDiagnosis of ImpactionMehek BatraAinda não há avaliações
- Leg PressDocumento4 páginasLeg PressAlfonso RobertAinda não há avaliações
- Nerve Compression (Entrapment) SyndromeDocumento23 páginasNerve Compression (Entrapment) SyndromeTrending razeAinda não há avaliações
- Thyroid ReportDocumento3 páginasThyroid ReportArman KhanAinda não há avaliações
- Effect of Kinesiotaping On Static and DyDocumento12 páginasEffect of Kinesiotaping On Static and DyMarcoAinda não há avaliações
- Mri Brain and Orbits: Name Age/Gender Ref. by MRN Report Date C-5-86311 Reg. DateDocumento2 páginasMri Brain and Orbits: Name Age/Gender Ref. by MRN Report Date C-5-86311 Reg. DateArslan MunawarAinda não há avaliações
- Cleft Lip and Palate Seminar Ed PDFDocumento100 páginasCleft Lip and Palate Seminar Ed PDFsaranyaazz100% (2)
- Aecep Fascia1Documento21 páginasAecep Fascia1Luis Fernando Ruiz Esparza AguileraAinda não há avaliações
- Thyroid Disorders: Dr. Lubna DwerijDocumento52 páginasThyroid Disorders: Dr. Lubna DwerijNoor MajaliAinda não há avaliações
- DA 5501 - Body Fat Content Worksheet (Female)Documento1 páginaDA 5501 - Body Fat Content Worksheet (Female)Kam 87Ainda não há avaliações
- REEMP AND SHIPBOARD REME Form B v4 20200730Documento1 páginaREEMP AND SHIPBOARD REME Form B v4 20200730Click TechnologyAinda não há avaliações
- Muscles of Facial Expression: Muscle Origin Insertion Action InnervationDocumento8 páginasMuscles of Facial Expression: Muscle Origin Insertion Action Innervationjameshouse100% (1)
- Autopsy Report: DECEDENT: John AndersonDocumento5 páginasAutopsy Report: DECEDENT: John AndersonjilliankadAinda não há avaliações
- Human Body Systems Essential VocabularyDocumento6 páginasHuman Body Systems Essential Vocabularyapi-261172766Ainda não há avaliações
- BJJ & MMA WorkoutsDocumento187 páginasBJJ & MMA WorkoutsVida BigbearAinda não há avaliações
- ACN - TCD Examination Techniques and InterpretationDocumento8 páginasACN - TCD Examination Techniques and InterpretationHanh NguyenAinda não há avaliações
- How To Squat - The Definitive Guide - Stronger by ScienceDocumento95 páginasHow To Squat - The Definitive Guide - Stronger by ScienceNilgunAinda não há avaliações
- Pathfit 1 Module 8 Week 10Documento28 páginasPathfit 1 Module 8 Week 10KrisChan ProdAinda não há avaliações