Você também pode gostar
- DystociaDocumento2 páginasDystociaPutri Rosalina TamzilAinda não há avaliações
- PRINT Untuk Lat OsceDocumento1 páginaPRINT Untuk Lat OscePutri Rosalina TamzilAinda não há avaliações
- Ophthalmic Procedures For Treatment of Advanced.8 PDFDocumento9 páginasOphthalmic Procedures For Treatment of Advanced.8 PDFPutri Rosalina TamzilAinda não há avaliações
- Ebook CampurDocumento2 páginasEbook CampurPutri Rosalina TamzilAinda não há avaliações
- Ophthalmic Dictionary and Vocabulary Builder For Eye Care ProfessionalsDocumento431 páginasOphthalmic Dictionary and Vocabulary Builder For Eye Care ProfessionalsPutri Rosalina TamzilAinda não há avaliações
- AAO Conjunctivitis PPPDocumento53 páginasAAO Conjunctivitis PPPjessicaceteAinda não há avaliações
- OSDI Questionnaire PDFDocumento2 páginasOSDI Questionnaire PDFPutri Rosalina TamzilAinda não há avaliações
- ArtefakDocumento7 páginasArtefakPutri Rosalina TamzilAinda não há avaliações
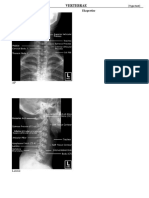
- Radiologi VertebraeDocumento12 páginasRadiologi VertebraePutri Rosalina TamzilAinda não há avaliações
- OsdiDocumento2 páginasOsdiFairuz PaiAinda não há avaliações
- Polikistik Kidney DiseaseDocumento9 páginasPolikistik Kidney DiseasesutrisnaarisAinda não há avaliações
- Arashi WishDocumento1 páginaArashi WishPutri Rosalina TamzilAinda não há avaliações
- OSDI Questionnaire PDFDocumento2 páginasOSDI Questionnaire PDFPutri Rosalina TamzilAinda não há avaliações
- JOI Vol 7 No 4 Des 2010 (Djajakusli S)Documento5 páginasJOI Vol 7 No 4 Des 2010 (Djajakusli S)IqaAinda não há avaliações
- The Work Limitations QuestionnaireDocumento14 páginasThe Work Limitations QuestionnairePutri Rosalina Tamzil100% (1)
- BR J Ophthalmol 2002 Lee 1347 51Documento6 páginasBR J Ophthalmol 2002 Lee 1347 51Putri Rosalina TamzilAinda não há avaliações
- A Small-Sample Survey of Dry Eye Symptoms Using The Ocular Surface Disease IndexDocumento4 páginasA Small-Sample Survey of Dry Eye Symptoms Using The Ocular Surface Disease IndexPutri Rosalina TamzilAinda não há avaliações
- Self-Reported Assessment of Dry Eye in A Population-Based Setting.Documento7 páginasSelf-Reported Assessment of Dry Eye in A Population-Based Setting.Putri Rosalina TamzilAinda não há avaliações
- Dry EyeDocumento11 páginasDry EyeFriedi Kristian Carlos100% (1)
- JOI Vol 7 No 4 Des 2010 (Djajakusli S)Documento5 páginasJOI Vol 7 No 4 Des 2010 (Djajakusli S)IqaAinda não há avaliações
- Dry Eye QuestionnaireDocumento2 páginasDry Eye QuestionnairePutri Rosalina TamzilAinda não há avaliações
- Work Productivity and Activity Impairment QuestionnaireDocumento4 páginasWork Productivity and Activity Impairment QuestionnairePutri Rosalina TamzilAinda não há avaliações
- Ai Ai Gasa by TegoMassDocumento2 páginasAi Ai Gasa by TegoMassPutri Rosalina TamzilAinda não há avaliações
- WPAI CodingDocumento1 páginaWPAI CodingPutri Rosalina TamzilAinda não há avaliações
- If NO, Check "NO" and Skip To Question 6Documento2 páginasIf NO, Check "NO" and Skip To Question 6FirmansahSaputraAinda não há avaliações
- ばれてる bare teru bare = to expose teru = to shine のに noni = although 堂々と doudou to = grandly/boldly 出れる to de reru = can I do/request some action はずない hazu nai = shouldn't たろう。 tarou. = probably doDocumento1 páginaばれてる bare teru bare = to expose teru = to shine のに noni = although 堂々と doudou to = grandly/boldly 出れる to de reru = can I do/request some action はずない hazu nai = shouldn't たろう。 tarou. = probably doPutri Rosalina TamzilAinda não há avaliações
- Review of Home Alone 2Documento3 páginasReview of Home Alone 2Putri Rosalina TamzilAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- A6 - Grp5 - Parenting Styles and Disciplinary Practices of Filipino Parents Towards Sex StereotypesDocumento51 páginasA6 - Grp5 - Parenting Styles and Disciplinary Practices of Filipino Parents Towards Sex StereotypesJM SarmientoAinda não há avaliações
- Business Plan Final Version (WIP) .Doc Change 5Documento54 páginasBusiness Plan Final Version (WIP) .Doc Change 5Hussain Chakera100% (1)
- A Research Study of Plastic Money Among HousewivesDocumento34 páginasA Research Study of Plastic Money Among HousewivesNainaAinda não há avaliações
- Exploring Hazard and Risk in Electrical Installation and Maintenance ORIGINALDocumento25 páginasExploring Hazard and Risk in Electrical Installation and Maintenance ORIGINALReymar PusaAinda não há avaliações
- Kaluuuuuuuuu FinalllllllllllDocumento33 páginasKaluuuuuuuuu Finalllllllllllevzy fernanadoAinda não há avaliações
- JMCM MethodologyDocumento29 páginasJMCM Methodologycclia CcAinda não há avaliações
- Redefining The Motivational Concepts Among Volunteers in The Context of The PhilippinesDocumento68 páginasRedefining The Motivational Concepts Among Volunteers in The Context of The PhilippinesJose PlazaAinda não há avaliações
- The Impact of Effective Forecasting On Business Growth, A Case of Businesses in Juba MarketDocumento17 páginasThe Impact of Effective Forecasting On Business Growth, A Case of Businesses in Juba MarketsegunAinda não há avaliações
- Master of Business Administration - MBA Semester 3 MB0034 Research Methodology - 3 Credits BKID: B0800Documento34 páginasMaster of Business Administration - MBA Semester 3 MB0034 Research Methodology - 3 Credits BKID: B0800kenguvaramuAinda não há avaliações
- Eappgrade12 q4 Week4 v4Documento17 páginasEappgrade12 q4 Week4 v4GLEZIEL-AN PIOCAinda não há avaliações
- Perception of Nursing Students On Clinical Learning EnvironmentDocumento6 páginasPerception of Nursing Students On Clinical Learning Environmentvodem79046Ainda não há avaliações
- Eapp - M7 - Stem12qDocumento1 páginaEapp - M7 - Stem12qsiahkyAinda não há avaliações
- The Likert Scale Revisited: An Alternate Version. (Product Preference Testing)Documento12 páginasThe Likert Scale Revisited: An Alternate Version. (Product Preference Testing)LucienAinda não há avaliações
- Data Collection MethodsDocumento82 páginasData Collection MethodsManjunath Shettigar73% (15)
- Coromandel International Fertilizers LimitedDocumento75 páginasCoromandel International Fertilizers LimitedpronoyalfiAinda não há avaliações
- ResearchDocumento22 páginasResearchAbegail BlancoAinda não há avaliações
- Module 3 Handout 1 12 Major Types of Research DesignsDocumento8 páginasModule 3 Handout 1 12 Major Types of Research DesignsShahbaz JadoonAinda não há avaliações
- Indahag National High School: Lesson Plan in Practical Research 2Documento2 páginasIndahag National High School: Lesson Plan in Practical Research 2Ruffa LAinda não há avaliações
- Practical Research 1 and 2Documento69 páginasPractical Research 1 and 2Lance Go LlanesAinda não há avaliações
- Sample Research From Last YearDocumento57 páginasSample Research From Last YearJasmin Rose GonzalesAinda não há avaliações
- Travel and Tour Business in ThamelDocumento45 páginasTravel and Tour Business in ThamelBeebek ChaudharyAinda não há avaliações
- Thesis Template (Numbered)Documento29 páginasThesis Template (Numbered)michaelurielAinda não há avaliações
- Final 103Documento55 páginasFinal 103Baesittieeleanor MamualasAinda não há avaliações
- Analyzing Perceived Writing Difficulties Through The Social Cognitive TheoryDocumento13 páginasAnalyzing Perceived Writing Difficulties Through The Social Cognitive TheoryGlobal Research and Development ServicesAinda não há avaliações
- Guano GRP 1Documento80 páginasGuano GRP 1Francielle EchanesAinda não há avaliações
- Cattle On Feed Report Dec. 23, 2022Documento10 páginasCattle On Feed Report Dec. 23, 2022Michael JohnsonAinda não há avaliações
- Evaluating The Satisfaction Factors of FPT University Student in "On-The-Job" Training ProgramDocumento15 páginasEvaluating The Satisfaction Factors of FPT University Student in "On-The-Job" Training ProgramJessaMaeDelosReyesAinda não há avaliações
- Social MediaDocumento11 páginasSocial MediaAldrinBalitaAinda não há avaliações
- KPI of Maintenance Management in Beverage IndustryDocumento8 páginasKPI of Maintenance Management in Beverage IndustryDon AndrianoAinda não há avaliações
- CONSUMER BUYING BEHAVIOR TOWARDS FASHION ACCESSORIES EYEWEAR Ijariie19005Documento7 páginasCONSUMER BUYING BEHAVIOR TOWARDS FASHION ACCESSORIES EYEWEAR Ijariie19005Kaushik SutradharAinda não há avaliações