Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- A Pocket Guide To Blood Pressure Measurement in ChildrenDocumento4 páginasA Pocket Guide To Blood Pressure Measurement in ChildrenKira23406Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Transel Buat FasDocumento3 páginasTransel Buat FasIchsani TamayaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Differential Diagnosis ReviewDocumento7 páginasDifferential Diagnosis ReviewSimina SerbanAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Diagnosis of Brain Death 2012 ARORADocumento71 páginasDiagnosis of Brain Death 2012 ARORAIchsani TamayaAinda não há avaliações
- NAP For Web - Headache Diagnosis TestingDocumento38 páginasNAP For Web - Headache Diagnosis TestingDeby Tri Widia LestariAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- 2012 JOSPT Guidelines LowBackPainDocumento58 páginas2012 JOSPT Guidelines LowBackPain1RogerioAinda não há avaliações
- Cheat WarcraftDocumento1 páginaCheat WarcraftArief RizkaAinda não há avaliações
- Your CallDocumento2 páginasYour CallIchsani TamayaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Bone DXR A OsteoarthritisDocumento11 páginasBone DXR A Osteoarthritisindra_poetoetAinda não há avaliações
- SEM Contract-Stephanie Medina PDFDocumento3 páginasSEM Contract-Stephanie Medina PDFStephanieAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Wan-Chi Chan ResumeDocumento1 páginaWan-Chi Chan Resumeapi-456456744Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- GZ Modifier ChartDocumento1 páginaGZ Modifier ChartvidhunenAinda não há avaliações
- BHLMP Form 1.b. Barangay Health System Development Six Building Block IndicatorsDocumento20 páginasBHLMP Form 1.b. Barangay Health System Development Six Building Block IndicatorsLouieAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Supply Chain Management in The Healthcare Sector: A Research AgendaDocumento6 páginasSupply Chain Management in The Healthcare Sector: A Research AgendaAbdul WahabAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- IHH Annual Report 2021 A PDFDocumento320 páginasIHH Annual Report 2021 A PDFPankaj DuttAinda não há avaliações
- Evidence Supports No Relationship Between Obstructive Sleep Apnea and Premolar Extraction: An Electronic Health Records ReviewDocumento6 páginasEvidence Supports No Relationship Between Obstructive Sleep Apnea and Premolar Extraction: An Electronic Health Records Revieworthodonticlit orthodonticlitAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Standards For Nursing EducationDocumento7 páginasStandards For Nursing Educationemir_bautista2002Ainda não há avaliações
- All India Hospital ListDocumento346 páginasAll India Hospital ListGnanaSai DattatreyaAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Scheduled Work Order Report - L3 - 2022-03-07T163611.767Documento1 páginaScheduled Work Order Report - L3 - 2022-03-07T163611.767Amin CrewAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- STT151A Long Quiz 3-1Documento4 páginasSTT151A Long Quiz 3-1Kasey LobregatAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- NCM 118 and 119 All Notes For ProcessingDocumento38 páginasNCM 118 and 119 All Notes For ProcessingBern NerquitAinda não há avaliações
- KSSHP Strategiakuva ENG - V01Documento2 páginasKSSHP Strategiakuva ENG - V01Shahnaz NawazAinda não há avaliações
- Guidelines For The Use of RH (D) Immunoglobulin (Anti D) (C Obs 6) Review November 2015Documento11 páginasGuidelines For The Use of RH (D) Immunoglobulin (Anti D) (C Obs 6) Review November 2015vasanthAinda não há avaliações
- DEMMI HandbookDocumento16 páginasDEMMI HandbookYamini DeenadayalanAinda não há avaliações
- Secondary - Technology Livelihood, Tech-Voc EducationDocumento24 páginasSecondary - Technology Livelihood, Tech-Voc EducationChona BontigaoAinda não há avaliações
- Aesthetics July 2015Documento72 páginasAesthetics July 2015Catalina Soler LioiAinda não há avaliações
- AVS Punarnava PPT - 12-02-2020Documento20 páginasAVS Punarnava PPT - 12-02-2020Sandeep ViswanathAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- English For Medicine II LI101002 Med: Khon Kaen University Language InstituteDocumento53 páginasEnglish For Medicine II LI101002 Med: Khon Kaen University Language InstituteSupanat TeerasuntornwongAinda não há avaliações
- State of The StateDocumento13 páginasState of The StateNews10NBCAinda não há avaliações
- AJACM 2009 4 1 Book ReviewsDocumento2 páginasAJACM 2009 4 1 Book ReviewsluyawinAinda não há avaliações
- Chief Supply Chain Officer 14Documento17 páginasChief Supply Chain Officer 14Bilal VirkAinda não há avaliações
- Mental Health ACT Terms and AbbreviationsDocumento2 páginasMental Health ACT Terms and AbbreviationsAsha ColmanAinda não há avaliações
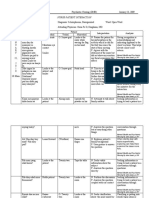
- Nurse-Patient Interaction: Mental Health and Psychiatric Nursing by Ann Isaacs p.197Documento4 páginasNurse-Patient Interaction: Mental Health and Psychiatric Nursing by Ann Isaacs p.197joey_gorgonioAinda não há avaliações
- Quality and Safety Walk Rounds A Co Designed Approach Toolkit and Case Study ReportDocumento52 páginasQuality and Safety Walk Rounds A Co Designed Approach Toolkit and Case Study ReportFederico GorgasAinda não há avaliações
- Np2 AnswerDocumento13 páginasNp2 AnswerMarie Jhoana100% (1)
- Treatment Options For Hyperemesis GravidarumDocumento11 páginasTreatment Options For Hyperemesis GravidarumJC QuinAinda não há avaliações
- Final Draft ResumeDocumento3 páginasFinal Draft Resumeapi-625242043Ainda não há avaliações
- Pci FormsDocumento13 páginasPci FormsKim SaludAinda não há avaliações
- Pharmacology DeptDocumento9 páginasPharmacology DeptNayan ChaudhariAinda não há avaliações