Você também pode gostar
- Osteoporosis MedscapeDocumento24 páginasOsteoporosis MedscapeMad MadAinda não há avaliações
- Living With Broken BonesDocumento56 páginasLiving With Broken BonesMad MadAinda não há avaliações
- Invivo Invitro AntioksidantDocumento14 páginasInvivo Invitro AntioksidantMad MadAinda não há avaliações
- Posology and Dosage RegimenDocumento24 páginasPosology and Dosage RegimenpmilyAinda não há avaliações
- Drug Treatments For OsteoporosisDocumento8 páginasDrug Treatments For OsteoporosisMad MadAinda não há avaliações
- NOGG Pocket Guide For Healthcare ProfessionalsDocumento10 páginasNOGG Pocket Guide For Healthcare ProfessionalsMad MadAinda não há avaliações
- Complementary and Alternative Therapies SEP 2013Documento5 páginasComplementary and Alternative Therapies SEP 2013Mad MadAinda não há avaliações
- Nejmoa1603800 2Documento14 páginasNejmoa1603800 2Mad MadAinda não há avaliações
- Spinal EpiduralDocumento8 páginasSpinal EpiduralMad MadAinda não há avaliações
- Treatment of Hypertension: JNC 8 and More: Pharmacist'S Letter / Prescriber'S LetterDocumento6 páginasTreatment of Hypertension: JNC 8 and More: Pharmacist'S Letter / Prescriber'S LetterJen CanlasAinda não há avaliações
- Mitos Danau TobaDocumento1 páginaMitos Danau TobaMad MadAinda não há avaliações
- Wild Mushroom ToxicologyDocumento5 páginasWild Mushroom ToxicologyMad MadAinda não há avaliações
- JurnalDocumento8 páginasJurnalMad MadAinda não há avaliações
- Cover LaporanDocumento2 páginasCover LaporanMad MadAinda não há avaliações
- A Randomized Trial of Intensive Versus Standard Blood-Pressure Control PDFDocumento14 páginasA Randomized Trial of Intensive Versus Standard Blood-Pressure Control PDFAnonymous 79KL9kAinda não há avaliações
- NeprologiDocumento5 páginasNeprologiMad MadAinda não há avaliações
- Serum Hepatitis BDocumento6 páginasSerum Hepatitis BMad MadAinda não há avaliações
- Ojmi 2013060415423580Documento4 páginasOjmi 2013060415423580Aden DhenAinda não há avaliações
- Perdosri MukernasDocumento26 páginasPerdosri MukernasMad MadAinda não há avaliações
- Metabolik ProfilDocumento15 páginasMetabolik ProfilMad MadAinda não há avaliações
- AnemiaDocumento10 páginasAnemiaMad MadAinda não há avaliações
- Metabolic SyndromeDocumento7 páginasMetabolic SyndromeMad MadAinda não há avaliações
- Pediatrik PlatinumDocumento5 páginasPediatrik PlatinumMad MadAinda não há avaliações
- TromboemboliDocumento7 páginasTromboemboliMad MadAinda não há avaliações
- Siduum ZirkoniumDocumento10 páginasSiduum ZirkoniumMad MadAinda não há avaliações
- Vitamin D Pada Anak EpilepsiDocumento7 páginasVitamin D Pada Anak EpilepsiMad MadAinda não há avaliações
- Genetic Diversity and Protectiv EfficacyDocumento13 páginasGenetic Diversity and Protectiv EfficacyMad MadAinda não há avaliações
- Novel Prion Disease AssociatedDocumento11 páginasNovel Prion Disease AssociatedMad MadAinda não há avaliações
- Asosiasi Vit DDocumento10 páginasAsosiasi Vit DMad MadAinda não há avaliações
- Serotonin InhibitorDocumento19 páginasSerotonin InhibitorMad MadAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Human Resouse Accounting Nature and Its ApplicationsDocumento12 páginasHuman Resouse Accounting Nature and Its ApplicationsParas JainAinda não há avaliações
- Practical Research 2: Self-Learning PackageDocumento3 páginasPractical Research 2: Self-Learning PackagePrinces BaccayAinda não há avaliações
- Exor EPF-1032 DatasheetDocumento2 páginasExor EPF-1032 DatasheetElectromateAinda não há avaliações
- sl2018 667 PDFDocumento8 páginassl2018 667 PDFGaurav MaithilAinda não há avaliações
- Antiquity: Middle AgesDocumento6 páginasAntiquity: Middle AgesPABLO DIAZAinda não há avaliações
- AtmDocumento6 páginasAtmAnkit JandialAinda não há avaliações
- (Variable Length Subnet MasksDocumento49 páginas(Variable Length Subnet MasksAnonymous GvIT4n41GAinda não há avaliações
- Self Team Assessment Form - Revised 5-2-20Documento6 páginasSelf Team Assessment Form - Revised 5-2-20api-630312626Ainda não há avaliações
- SEO Design ExamplesDocumento10 páginasSEO Design ExamplesAnonymous YDwBCtsAinda não há avaliações
- Deep Groove Ball Bearings PDFDocumento11 páginasDeep Groove Ball Bearings PDFArpit VermaAinda não há avaliações
- Emergency Room Delivery RecordDocumento7 páginasEmergency Room Delivery RecordMariel VillamorAinda não há avaliações
- Brain, Behavior, and Immunity: Alok Kumar, David J. LoaneDocumento11 páginasBrain, Behavior, and Immunity: Alok Kumar, David J. LoaneRinaldy TejaAinda não há avaliações
- ASTM D256-10 - Standard Test Methods For Determining The Izod Pendulum Impact Resistance of PlasticsDocumento20 páginasASTM D256-10 - Standard Test Methods For Determining The Izod Pendulum Impact Resistance of PlasticsEng. Emílio DechenAinda não há avaliações
- Material Safety Data Sheet Lime Kiln Dust: Rev. Date:5/1/2008Documento6 páginasMaterial Safety Data Sheet Lime Kiln Dust: Rev. Date:5/1/2008suckrindjink100% (1)
- National Advisory Committee For AeronauticsDocumento36 páginasNational Advisory Committee For AeronauticsSamuel ChristioAinda não há avaliações
- Yanmar America publication listing for engine parts, service, and operation manualsDocumento602 páginasYanmar America publication listing for engine parts, service, and operation manualsEnrique Murgia50% (2)
- Reservoir Rock TypingDocumento56 páginasReservoir Rock TypingAffan HasanAinda não há avaliações
- ĐỀ SỐ 3Documento5 páginasĐỀ SỐ 3Thanhh TrúcAinda não há avaliações
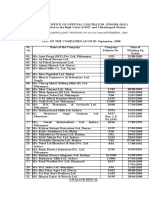
- Statement of Compulsory Winding Up As On 30 SEPTEMBER, 2008Documento4 páginasStatement of Compulsory Winding Up As On 30 SEPTEMBER, 2008abchavhan20Ainda não há avaliações
- Living Nonliving DeadDocumento11 páginasLiving Nonliving DeadArun AcharyaAinda não há avaliações
- Liber Chao (Final - Eng)Documento27 páginasLiber Chao (Final - Eng)solgrae8409100% (2)
- Standard Deviation IntroductionDocumento3 páginasStandard Deviation IntroductionShyam ShresthaAinda não há avaliações
- Employee Engagement A Case Study at IVRCL-1Documento7 páginasEmployee Engagement A Case Study at IVRCL-1Anonymous dozzql7znKAinda não há avaliações
- NOTE CHAPTER 3 The Mole Concept, Chemical Formula and EquationDocumento10 páginasNOTE CHAPTER 3 The Mole Concept, Chemical Formula and EquationNur AfiqahAinda não há avaliações
- IP68 Rating ExplainedDocumento12 páginasIP68 Rating ExplainedAdhi ErlanggaAinda não há avaliações
- Socially Responsible CompaniesDocumento2 páginasSocially Responsible CompaniesItzman SánchezAinda não há avaliações
- Periodic ClassificationDocumento4 páginasPeriodic ClassificationtusharAinda não há avaliações
- Supreme Court rules stabilization fees not trust fundsDocumento8 páginasSupreme Court rules stabilization fees not trust fundsNadzlah BandilaAinda não há avaliações
- Environmental Assessment of Sewer ConstructionDocumento32 páginasEnvironmental Assessment of Sewer ConstructionKaleab TadesseAinda não há avaliações
- Vehicle Registration Renewal Form DetailsDocumento1 páginaVehicle Registration Renewal Form Detailsabe lincolnAinda não há avaliações