Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- GaN technology powers bright LEDsDocumento13 páginasGaN technology powers bright LEDsluciowwAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- SHB 2503-3703 en 1000081433Documento192 páginasSHB 2503-3703 en 1000081433Alberto100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Nature of Acidity and Lime Requirement in Acid Soils of ManipurDocumento8 páginasNature of Acidity and Lime Requirement in Acid Soils of ManipurIJASRETAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- As 4123.4-2008 Mobile Waste Containers Containers With Four Wheels With A Capacity From 750 L To 1700 L WithDocumento7 páginasAs 4123.4-2008 Mobile Waste Containers Containers With Four Wheels With A Capacity From 750 L To 1700 L WithSAI Global - APACAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Deventer04 MACDocumento201 páginasDeventer04 MACFrancisco Solano Reyes EspinozaAinda não há avaliações
- EGIG - 10th - Report - Final - 09-03-2018 - v1Documento50 páginasEGIG - 10th - Report - Final - 09-03-2018 - v1Paulo Marcos Cabral JuniorAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- STN Cat Novelties Vol.i 2023Documento89 páginasSTN Cat Novelties Vol.i 2023ruba herbawiAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- LV12 - Drive Shafts - Issue 1Documento19 páginasLV12 - Drive Shafts - Issue 1Đức HòangAinda não há avaliações
- Resume of MD Saiful HyderDocumento4 páginasResume of MD Saiful Hyderimtheboss*Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Network What To ReadDocumento2 páginasNetwork What To ReadTauseef AhmadAinda não há avaliações
- 2022 Manufacture AnswerDocumento8 páginas2022 Manufacture AnswerChampika V SamarasighaAinda não há avaliações
- CV Enric Durany enDocumento2 páginasCV Enric Durany enenricduranyAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
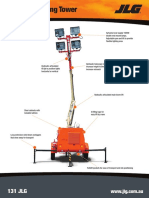
- JLG Lighting Tower 6308AN Series II 20150907Documento2 páginasJLG Lighting Tower 6308AN Series II 20150907DwiSulistyo09Ainda não há avaliações
- NPTEL Science and Technology of PolymersDocumento2 páginasNPTEL Science and Technology of PolymersAzhagiri PonAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- FG - BDER-78 Technical Catalogue - Technical - UNDocumento8 páginasFG - BDER-78 Technical Catalogue - Technical - UNAnh Le NgocAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Design of A Fluidized Drum GranulatorDocumento6 páginasDesign of A Fluidized Drum GranulatorditchcheAinda não há avaliações
- Coco Press KitDocumento55 páginasCoco Press KitPaula RiddenAinda não há avaliações
- PHP AngularJS CRUD with Search and PaginationDocumento18 páginasPHP AngularJS CRUD with Search and PaginationZaiful BahriAinda não há avaliações
- Unit Conversion Heat TransferDocumento5 páginasUnit Conversion Heat TransferFamela GadAinda não há avaliações
- Ps 1 SolDocumento3 páginasPs 1 SolPang XsAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Niveau S Longrine Type Pou05-S Section 20x25: A-A B-B C-C D-DDocumento1 páginaNiveau S Longrine Type Pou05-S Section 20x25: A-A B-B C-C D-DAWOUNANGAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Correlation Study and Regression Analysis of Water Quality Assessment of Nagpur City, IndiaDocumento5 páginasCorrelation Study and Regression Analysis of Water Quality Assessment of Nagpur City, IndiaShakeel AhmadAinda não há avaliações
- Method Statement For Architecture Work (Drywall) : No. Work Sequence Good Practices Picture Tools RemarksDocumento16 páginasMethod Statement For Architecture Work (Drywall) : No. Work Sequence Good Practices Picture Tools RemarksAn-an ChanAinda não há avaliações
- Communication System (LC-ECE204G) LAB ManualDocumento54 páginasCommunication System (LC-ECE204G) LAB ManualBindia HandaAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- INTERCOMP Pt300 Users Manual Rev GDocumento44 páginasINTERCOMP Pt300 Users Manual Rev GCTN2010Ainda não há avaliações
- RCC BEAM DESIGN AND SERVICEABILITYDocumento15 páginasRCC BEAM DESIGN AND SERVICEABILITYprashmceAinda não há avaliações
- Caterpillar 914GDocumento28 páginasCaterpillar 914GForomaquinas100% (3)
- ETN2A ElectromechanicsDocumento64 páginasETN2A ElectromechanicsEinstein's VanderbijlparkAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- 1855OME - Instruction Manual - Kinney Oil Mist EliminatorsDocumento15 páginas1855OME - Instruction Manual - Kinney Oil Mist EliminatorsahmedAinda não há avaliações