Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Checklist Persiapan Operasional Emergency Department: Sheet1Documento10 páginasChecklist Persiapan Operasional Emergency Department: Sheet1Jose Hady PuteraAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
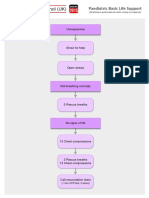
- Paediatric Basic Life Support: UnresponsiveDocumento1 páginaPaediatric Basic Life Support: UnresponsiveJose Hady PuteraAinda não há avaliações
- Rna Virus Rna VirusDocumento2 páginasRna Virus Rna VirusJose Hady PuteraAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Dna Virus Dna VirusDocumento2 páginasDna Virus Dna VirusJose Hady PuteraAinda não há avaliações
- Body Surface Area Body Surface AreaDocumento4 páginasBody Surface Area Body Surface AreaJose Hady PuteraAinda não há avaliações
- Komplikasi Stroke PDFDocumento7 páginasKomplikasi Stroke PDFJose Hady PuteraAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- JZBQYB Cara Lainnya Juga Bisa Dilakukan DenganDocumento2 páginasJZBQYB Cara Lainnya Juga Bisa Dilakukan DenganJose Hady PuteraAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- My First Authored PublicationDocumento16 páginasMy First Authored PublicationSamuel UzonduAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- NPB 168 Practice Exam 2Documento5 páginasNPB 168 Practice Exam 2Kim Wong100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- TRIKATUDocumento5 páginasTRIKATUAngshuman DuttaAinda não há avaliações
- PranoyDocumento24 páginasPranoySupriyo ChatterjeeAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Incision and Drainage of AbscessesDocumento25 páginasIncision and Drainage of Abscessesjaphetnwapi100% (1)
- Endorsement Template SURGERYDocumento2 páginasEndorsement Template SURGERYElizalde HusbandAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Operating RoomDocumento51 páginasOperating RoomKasnhaAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Medical Needs Fatiguing The Descrpit Social CcienceDocumento11 páginasMedical Needs Fatiguing The Descrpit Social Ccienceicicle900Ainda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- National Quality Assurance Standards: Mandatory Requirements PHC/CHCDocumento14 páginasNational Quality Assurance Standards: Mandatory Requirements PHC/CHCSathish KumaarAinda não há avaliações
- Electrolyte ReplacementDocumento3 páginasElectrolyte ReplacementRatih Dwi OctariaAinda não há avaliações
- Flower Horn DiseasesDocumento4 páginasFlower Horn DiseasesSandeep ModiAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Regulatory Compliance Pharmacy Manager in Tampa FL Resume John HawesDocumento2 páginasRegulatory Compliance Pharmacy Manager in Tampa FL Resume John HawesJohnHawesAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- PACS Basics PDFDocumento6 páginasPACS Basics PDFBalaji BalasubramanianAinda não há avaliações
- Sexual Behaviors in Autism: Problems of Definition and ManagementDocumento7 páginasSexual Behaviors in Autism: Problems of Definition and ManagementPaula MarcuAinda não há avaliações
- Faculty 363 Histotechnique Lectures - 2Documento27 páginasFaculty 363 Histotechnique Lectures - 2einsteinspy100% (1)
- USMLE - VirusesDocumento120 páginasUSMLE - Viruseszeal7777100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Induction Update2Documento30 páginasInduction Update2yusepAinda não há avaliações
- Personal Accident Claim Form: Particulars of Insured (Company / Individual)Documento2 páginasPersonal Accident Claim Form: Particulars of Insured (Company / Individual)Robbie Chan100% (1)
- HIV and PregnancyDocumento9 páginasHIV and PregnancyUm HamoOdAinda não há avaliações
- By - Derina FixDocumento1 páginaBy - Derina FixSellyta HasugianAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Hirayama Disease and HomoeopathyDocumento11 páginasHirayama Disease and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (3)
- Folliculitis Decalvans Update July 2019 - Lay Reviewed July 2019Documento4 páginasFolliculitis Decalvans Update July 2019 - Lay Reviewed July 2019sjeyarajah21Ainda não há avaliações
- Pest ControlDocumento8 páginasPest ControlFirst Last100% (1)
- PRACTICE GUIDELINE For The Treatment of Patients With SchizophreniaDocumento184 páginasPRACTICE GUIDELINE For The Treatment of Patients With SchizophreniabencortesmoralesAinda não há avaliações
- Orthotic/Prosthetic Referral Form: Dispensing RX: Please Evaluate and Treat Patient With The Following DeviceDocumento1 páginaOrthotic/Prosthetic Referral Form: Dispensing RX: Please Evaluate and Treat Patient With The Following DeviceKelly Roberts WiggenAinda não há avaliações
- Stem Cell Research PaperDocumento3 páginasStem Cell Research Papermyrentistoodamnhigh100% (1)
- Strength Training & Weight Training 101Documento28 páginasStrength Training & Weight Training 101Maru PabloAinda não há avaliações
- Site-Specific and Stoichiometric Modification of Antibodies by Bacterial TransglutaminaseDocumento3 páginasSite-Specific and Stoichiometric Modification of Antibodies by Bacterial Transglutaminasespamemail00Ainda não há avaliações
- Mommy's MedicineDocumento3 páginasMommy's Medicinekcs.crimsonfoxAinda não há avaliações
- Trends of Violence Against Healthcare by ShaheerDocumento9 páginasTrends of Violence Against Healthcare by ShaheerShaheer zia100% (1)