Você também pode gostar
- PLAB 1700 MCQs Dr. Khalid - S Explanation of 1700 MCQDocumento680 páginasPLAB 1700 MCQs Dr. Khalid - S Explanation of 1700 MCQguzelnor100% (35)
- Myofascial Trigger PointsDocumento17 páginasMyofascial Trigger PointsVera Belchior100% (3)
- Lower GI Bleeding SlideDocumento29 páginasLower GI Bleeding Slideraed faisalAinda não há avaliações
- Cardiac OutputDocumento37 páginasCardiac OutputIndrashish Chakravorty100% (1)
- Floppy BabyDocumento13 páginasFloppy BabyJorge JhgAinda não há avaliações
- Abdomen ExaminationDocumento37 páginasAbdomen ExaminationJaaydevAinda não há avaliações
- Hematemesis Melena (Upper Gi Bleeding)Documento134 páginasHematemesis Melena (Upper Gi Bleeding)Mardoni Efrijon100% (1)
- Portal Hypertension - A Case ReportDocumento65 páginasPortal Hypertension - A Case ReportTEAM K 1920Ainda não há avaliações
- Fat EmbolismDocumento12 páginasFat EmbolismHastina HadnanAinda não há avaliações
- Injuries To Genitourinary TractDocumento130 páginasInjuries To Genitourinary TractYUFFAAinda não há avaliações
- Approach To The Patient With Endocrine DisordersDocumento17 páginasApproach To The Patient With Endocrine Disordersseun williamsAinda não há avaliações
- Upper and Lower GI Bleeding Differential DiagnosesDocumento3 páginasUpper and Lower GI Bleeding Differential DiagnosesKEn PilapilAinda não há avaliações
- Anesthesia: Mrs - SanthiDocumento59 páginasAnesthesia: Mrs - SanthisanthiyasandyAinda não há avaliações
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Patient Safety Awareness Course Test 2017Documento5 páginasPatient Safety Awareness Course Test 2017MochaLover0% (1)
- Palliative Care Pain and Symptom Control GuidelinesDocumento128 páginasPalliative Care Pain and Symptom Control GuidelinesAQSA AHMED SIDDIQUIAinda não há avaliações
- Fluid and ElectrolytesDocumento107 páginasFluid and ElectrolytesStephenus JavedAinda não há avaliações
- CWU OrthopedicsDocumento6 páginasCWU OrthopedicsSana Anam JahanAinda não há avaliações
- Question and Answers For MFD OSCE ExaminationDocumento15 páginasQuestion and Answers For MFD OSCE ExaminationAmeer Fadel100% (1)
- Compartment-Syndrome PPT GADAR 2Documento20 páginasCompartment-Syndrome PPT GADAR 2meikha tari batjun0% (1)
- Explanation LetterDocumento1 páginaExplanation LettersaufisafingiAinda não há avaliações
- Intensive Care Medicine MCQs Multiple Choice Questions With Explanatory AnswersDocumento350 páginasIntensive Care Medicine MCQs Multiple Choice Questions With Explanatory AnswersHiago Sousa59% (17)
- Breast ExamDocumento4 páginasBreast Exammoony_sasAinda não há avaliações
- Medical Gases SupplyDocumento6 páginasMedical Gases SupplyManuela PascalAinda não há avaliações
- Hanson Infectious Diseases - Anamneza I StatusDocumento33 páginasHanson Infectious Diseases - Anamneza I StatusSilvia KesegAinda não há avaliações
- Guia Gold Epoc 2022Documento177 páginasGuia Gold Epoc 2022Maria Jose CastilloAinda não há avaliações
- Robotic SurgeryDocumento33 páginasRobotic SurgeryGauri Priya RohithAinda não há avaliações
- Disseminated Intravascular Coagulation - Background, Pathophysiology, EtiologyDocumento11 páginasDisseminated Intravascular Coagulation - Background, Pathophysiology, Etiologyevi100% (2)
- Day Care SurgeryDocumento5 páginasDay Care SurgeryazharmoAinda não há avaliações
- Upper GIT BleedingDocumento69 páginasUpper GIT BleedingSoleh Ramly100% (1)
- Discuss Day Case SurgeryDocumento28 páginasDiscuss Day Case SurgeryrosybashAinda não há avaliações
- Fractional RF Machine: Use InstructionDocumento21 páginasFractional RF Machine: Use Instructionjuras500Ainda não há avaliações
- ConvoDocumento44 páginasConvoLun Ding0% (1)
- Thyroid Neoplasms: Kelompok 3 Dr. Reza Maulana Dr. Intan E. Napitupulu Drg. Andi Arfandi ArifuddinDocumento41 páginasThyroid Neoplasms: Kelompok 3 Dr. Reza Maulana Dr. Intan E. Napitupulu Drg. Andi Arfandi ArifuddinIntan Eklesiana NapitupuluAinda não há avaliações
- Biostatistics: Long Quiz Key AnswerDocumento9 páginasBiostatistics: Long Quiz Key Answeraleah ternalAinda não há avaliações
- Differential Diagnosis of Abdominal Pain in AdultsDocumento18 páginasDifferential Diagnosis of Abdominal Pain in AdultsTe HineahuoneAinda não há avaliações
- Murmur EvaluationDocumento4 páginasMurmur EvaluationManjunath GeminiAinda não há avaliações
- Course in The WardDocumento3 páginasCourse in The WardAljon S. TemploAinda não há avaliações
- Antibiotics in SurgeryDocumento18 páginasAntibiotics in SurgeryGiovanni HenryAinda não há avaliações
- Mangled Extremity and TreatmentDocumento37 páginasMangled Extremity and TreatmentrakanootousanAinda não há avaliações
- Massive Blood TransfusionDocumento17 páginasMassive Blood TransfusionevanAinda não há avaliações
- Phyllodes Tumors of The Breast UpToDateDocumento22 páginasPhyllodes Tumors of The Breast UpToDateSean SialanaAinda não há avaliações
- Lecture Notes On Surgery - Part II - Dr. Yogiram BolisettyDocumento79 páginasLecture Notes On Surgery - Part II - Dr. Yogiram Bolisettyjun sianAinda não há avaliações
- Inguino Scrotal SwellingDocumento3 páginasInguino Scrotal SwellingYurni Dwi AstutiAinda não há avaliações
- Deep Vein ThrombosisDocumento24 páginasDeep Vein ThrombosisdinafiniAinda não há avaliações
- EpendymomaDocumento5 páginasEpendymomaDenny's BerciaAinda não há avaliações
- Acute Post Streptococcal Glomerulonephritis APSGNDocumento16 páginasAcute Post Streptococcal Glomerulonephritis APSGNErlin IrawatiAinda não há avaliações
- Wound AssessmentDocumento5 páginasWound AssessmentJake EverettAinda não há avaliações
- SurgeryDocumento12 páginasSurgeryManusheeAinda não há avaliações
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDocumento25 páginasSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13Ainda não há avaliações
- Factors Affectin Block HeightDocumento37 páginasFactors Affectin Block HeightshikhaAinda não há avaliações
- Bag Valve MaskDocumento4 páginasBag Valve MaskMiguel BascunanAinda não há avaliações
- Management of Acute Appendicitis in Adults - UpToDateDocumento28 páginasManagement of Acute Appendicitis in Adults - UpToDateaulia rachman100% (1)
- Polycythemia VeraDocumento22 páginasPolycythemia VeraMelisande Rae CiruelaAinda não há avaliações
- General Surgery TextbookDocumento25 páginasGeneral Surgery TextbookIsak Isak IsakAinda não há avaliações
- Perforated Peptic UlcerDocumento68 páginasPerforated Peptic UlcerSaibo BoldsaikhanAinda não há avaliações
- Concept Map MI 2Documento1 páginaConcept Map MI 2nicole barcenaAinda não há avaliações
- Abdominal Pain - Pathophysiology, Classification and CausesDocumento8 páginasAbdominal Pain - Pathophysiology, Classification and CausesdanukamajayaAinda não há avaliações
- GERD SchwartzDocumento10 páginasGERD SchwartzMina Tharwat AzerAinda não há avaliações
- Adverse Effects of Blood TransfusionsDocumento3 páginasAdverse Effects of Blood Transfusionsay254Ainda não há avaliações
- MEDIATRIXDocumento67 páginasMEDIATRIXMaria Consuelo LingcasoAinda não há avaliações
- Fast HugDocumento41 páginasFast HugBharti NaraAinda não há avaliações
- Acute AppendicitisDocumento17 páginasAcute AppendicitisMukhtar Khan0% (1)
- Stevens Johnson DiseaseDocumento5 páginasStevens Johnson DiseaseShammy RNAinda não há avaliações
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDocumento2 páginasAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasAinda não há avaliações
- Approach To The Adult Patient With Anemia - UpToDateDocumento23 páginasApproach To The Adult Patient With Anemia - UpToDateNicole SierraAinda não há avaliações
- CholecystectomyDocumento4 páginasCholecystectomySoheil LimboAinda não há avaliações
- Procedure and Equipment OrthopedicDocumento29 páginasProcedure and Equipment OrthopedicKah Man GohAinda não há avaliações
- SCI & Cauda Equina SyndromeDocumento14 páginasSCI & Cauda Equina SyndromeKah Man GohAinda não há avaliações
- Clinical Audit For Rejected Bloos Specimen (Autosaved)Documento22 páginasClinical Audit For Rejected Bloos Specimen (Autosaved)Kah Man GohAinda não há avaliações
- Transfusion Reaction PDFDocumento1 páginaTransfusion Reaction PDFKah Man GohAinda não há avaliações
- Transfusion Reaction PDFDocumento1 páginaTransfusion Reaction PDFKah Man GohAinda não há avaliações
- Answers For MMS On BBB - Headache-Raised ICPDocumento2 páginasAnswers For MMS On BBB - Headache-Raised ICPKah Man GohAinda não há avaliações
- Liver Function TestDocumento10 páginasLiver Function TestKah Man GohAinda não há avaliações
- Toward Competency-Based Medical Education: PerspectiveDocumento3 páginasToward Competency-Based Medical Education: PerspectiveKah Man GohAinda não há avaliações
- SpleenAnatomy Functions Rupture HypersplenismDocumento77 páginasSpleenAnatomy Functions Rupture HypersplenismKah Man GohAinda não há avaliações
- Diabetic Retinopathy Case 09Documento2 páginasDiabetic Retinopathy Case 09Kah Man GohAinda não há avaliações
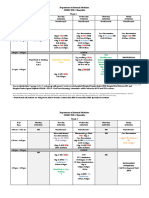
- Semester 6 Timetable 25 April 2016 To 10 June 2016 (GRP C) Revised 12 May 2016Documento7 páginasSemester 6 Timetable 25 April 2016 To 10 June 2016 (GRP C) Revised 12 May 2016Kah Man GohAinda não há avaliações
- IMS Group A Sem 5 Abnormal Liver FunctionDocumento30 páginasIMS Group A Sem 5 Abnormal Liver FunctionKah Man GohAinda não há avaliações
- TST Prep - 100 TOEFL Reading Practice Questions-110-120Documento11 páginasTST Prep - 100 TOEFL Reading Practice Questions-110-120S EAinda não há avaliações
- Syrgery Mock 10Documento8 páginasSyrgery Mock 10Sergiu CiobanuAinda não há avaliações
- Perioperative Concepts and Nursing Management: NCM 112-LecturerDocumento98 páginasPerioperative Concepts and Nursing Management: NCM 112-LecturerJaylord Verazon100% (1)
- Unit 2 - Innovations in Health and Medicine (Paragraphs)Documento1 páginaUnit 2 - Innovations in Health and Medicine (Paragraphs)April ThunAinda não há avaliações
- Hiddensee - Michelle HartDocumento13 páginasHiddensee - Michelle HartviniciuscarpeAinda não há avaliações
- Amniotic MembraneDocumento8 páginasAmniotic Membraneapi-481789048Ainda não há avaliações
- MsdsDocumento6 páginasMsdsEris AgustinAinda não há avaliações
- Biology Form 4 Chapter 5 Cell DivisionDocumento7 páginasBiology Form 4 Chapter 5 Cell Divisiongelgaban67% (3)
- A2 - Practice 29Documento2 páginasA2 - Practice 29123VinhcuuAinda não há avaliações
- Blood Transfusion Reactions: P Sunil Kumar Department of Haematology ST - John's Medical CollegeDocumento48 páginasBlood Transfusion Reactions: P Sunil Kumar Department of Haematology ST - John's Medical CollegeFULGENCE RUHARARAAinda não há avaliações
- Guidelines On NADOPOD Regulations 2004Documento28 páginasGuidelines On NADOPOD Regulations 2004LuqmanAlHakimAinda não há avaliações
- Overview of AntibioticsDocumento5 páginasOverview of AntibioticsakshahinbdAinda não há avaliações
- Lethal Midline Granuloma-Stewart Nasal Nk/T-Cell Lymphoma-0ur ExperienceDocumento9 páginasLethal Midline Granuloma-Stewart Nasal Nk/T-Cell Lymphoma-0ur Experienceopi akbarAinda não há avaliações
- Master / Fernandes How To Study Materia Medica?: Reading ExcerptDocumento5 páginasMaster / Fernandes How To Study Materia Medica?: Reading ExcerptKarthikAinda não há avaliações
- Mosquito Net SpecificationDocumento12 páginasMosquito Net SpecificationManoj KumarAinda não há avaliações
- 常用詞彙表Documento10 páginas常用詞彙表GXAinda não há avaliações
- SAMPLE ELC151 - Final - TEST - PDFDocumento11 páginasSAMPLE ELC151 - Final - TEST - PDFNara SakuraAinda não há avaliações
- EMCrit Lae Pulmonary FlowDocumento1 páginaEMCrit Lae Pulmonary FlowhmsptrAinda não há avaliações
- A Simple Approach To Shared Decision Making in Cancer ScreeningDocumento6 páginasA Simple Approach To Shared Decision Making in Cancer ScreeningariskaAinda não há avaliações
- Prognostic Factors and Management of Patients With Choanal AtresiaDocumento7 páginasPrognostic Factors and Management of Patients With Choanal Atresiafarah maulida martaAinda não há avaliações
- Case Study 416Documento34 páginasCase Study 416jennifer_crumm100% (1)
- Nutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsDocumento15 páginasNutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsIOSRjournalAinda não há avaliações
- Sociology PresentationDocumento31 páginasSociology PresentationNirbhay SinghAinda não há avaliações
- NearfatalasthmaDocumento8 páginasNearfatalasthmaHeath HensleyAinda não há avaliações
- Lymphatic Filariasis Life Cycle PDFDocumento1 páginaLymphatic Filariasis Life Cycle PDFlauraAinda não há avaliações