Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Seventh Day Adventist Quiz by KnowingTheTimeDocumento4 páginasSeventh Day Adventist Quiz by KnowingTheTimeMiiiTheart100% (3)
- Clinical Significance of Accessory Foramina in AduDocumento6 páginasClinical Significance of Accessory Foramina in AduAndrea LawAinda não há avaliações
- Tetric LineDocumento10 páginasTetric LineAndrea LawAinda não há avaliações
- Dental WaxDocumento2 páginasDental WaxAndrea LawAinda não há avaliações
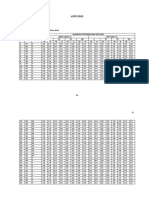
- Appendix: Appendix 1 Master Table Alveolar Bone Resorption DataDocumento12 páginasAppendix: Appendix 1 Master Table Alveolar Bone Resorption DataAndrea LawAinda não há avaliações
- Bab 5Documento1 páginaBab 5Andrea LawAinda não há avaliações
- Dental WaxDocumento14 páginasDental WaxAndrea LawAinda não há avaliações
- 5 CementoenamelDocumento8 páginas5 CementoenamelAndrea LawAinda não há avaliações
- Young Practitioners Guide To PeriodontologyDocumento36 páginasYoung Practitioners Guide To PeriodontologyAndrea Law100% (3)
- Index of RefractionDocumento3 páginasIndex of RefractionAndrea LawAinda não há avaliações
- Example Adult Maxillary Anterior Occlusal Radiograph.: SourceDocumento2 páginasExample Adult Maxillary Anterior Occlusal Radiograph.: SourceAndrea LawAinda não há avaliações
- Terms:: 1) HypoplasticDocumento3 páginasTerms:: 1) HypoplasticAndrea LawAinda não há avaliações
- The Function of TongueDocumento11 páginasThe Function of TongueAndrea LawAinda não há avaliações
- Travel Smart: Assignment 1: Project ProposalDocumento14 páginasTravel Smart: Assignment 1: Project ProposalcattytomeAinda não há avaliações
- Edgardo Macabulos - FS1-Activity-1Documento8 páginasEdgardo Macabulos - FS1-Activity-1Macabulos Edgardo SableAinda não há avaliações
- Anthropology Chapter 2 ADocumento17 páginasAnthropology Chapter 2 AHafiz SaadAinda não há avaliações
- Mejia V Reyes - DumaguingDocumento1 páginaMejia V Reyes - DumaguingRonalyn GaculaAinda não há avaliações
- Timing Light Schematic or DiagramDocumento2 páginasTiming Light Schematic or Diagramprihharmanto antokAinda não há avaliações
- SAP Workflow Scenario: Maintenance Notification ApprovalDocumento6 páginasSAP Workflow Scenario: Maintenance Notification ApprovalPiyush BoseAinda não há avaliações
- ART 6 LEARNING PACKET Week2-3Documento10 páginasART 6 LEARNING PACKET Week2-3Eljohn CabantacAinda não há avaliações
- Henry FayolDocumento4 páginasHenry FayolFaryal MughalAinda não há avaliações
- Equal Protection and Public Education EssayDocumento6 páginasEqual Protection and Public Education EssayAccount YanguAinda não há avaliações
- Tate J. Hedtke SPED 608 Assignment #6 Standard # 8 Cross Categorical Special Education/ Learning Disabilities Artifact SummaryDocumento5 páginasTate J. Hedtke SPED 608 Assignment #6 Standard # 8 Cross Categorical Special Education/ Learning Disabilities Artifact Summaryapi-344731850Ainda não há avaliações
- Barclays Global FX Quarterly Fed On Hold Eyes On GrowthDocumento42 páginasBarclays Global FX Quarterly Fed On Hold Eyes On GrowthgneymanAinda não há avaliações
- Writing Ielts Tasks Andreea ReviewDocumento18 páginasWriting Ielts Tasks Andreea ReviewRody BudeșAinda não há avaliações
- Axis Bank - Hoam LoanDocumento21 páginasAxis Bank - Hoam LoansonamAinda não há avaliações
- 3.1 Learning To Be A Better StudentDocumento27 páginas3.1 Learning To Be A Better StudentApufwplggl JomlbjhfAinda não há avaliações
- Reaction PaperDocumento4 páginasReaction PaperCeñidoza Ian AlbertAinda não há avaliações
- RARC Letter To Tan Seri Razali Ismail July 26-2013Documento4 páginasRARC Letter To Tan Seri Razali Ismail July 26-2013Rohingya VisionAinda não há avaliações
- Compare and Contrast Two Cultures Celebrate Between Bali and JavaDocumento1 páginaCompare and Contrast Two Cultures Celebrate Between Bali and JavaqonitazmiAinda não há avaliações
- Lolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad MedinaceliDocumento3 páginasLolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad Medinacelichatmche-06Ainda não há avaliações
- Percussion Digital TWDocumento26 páginasPercussion Digital TWAlberto GallardoAinda não há avaliações
- Pugh MatrixDocumento18 páginasPugh MatrixSulaiman Khan0% (1)
- Ramin Shamshiri Risk Analysis Exam2 PDFDocumento8 páginasRamin Shamshiri Risk Analysis Exam2 PDFRedmond R. ShamshiriAinda não há avaliações
- Anglicanism QuestionsDocumento36 páginasAnglicanism QuestionsspringsdanielconceptAinda não há avaliações
- WLAS - CSS 12 - w3Documento11 páginasWLAS - CSS 12 - w3Rusty Ugay LumbresAinda não há avaliações
- What Is Art?Documento14 páginasWhat Is Art?Sarvenaaz QaffariAinda não há avaliações
- Exam Note NegligenceDocumento15 páginasExam Note Negligenceengyi96Ainda não há avaliações
- He Didnt Die in Vain - Take No GloryDocumento2 páginasHe Didnt Die in Vain - Take No GloryDagaerag Law OfficeAinda não há avaliações
- Schmitt Allik 2005 ISDP Self Esteem - 000 PDFDocumento20 páginasSchmitt Allik 2005 ISDP Self Esteem - 000 PDFMariana KapetanidouAinda não há avaliações
- Functions of Communication Oral Communication PDFDocumento12 páginasFunctions of Communication Oral Communication PDFKrystle Francess Barrios0% (1)
- Network Firewall SecurityDocumento133 páginasNetwork Firewall Securitysagar323Ainda não há avaliações