Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- 101 Freedom SampleDocumento10 páginas101 Freedom Sampleshetalksloud100% (1)
- Poetry Rehab - A Poetry Anthology On The Journey To RecoveryDocumento37 páginasPoetry Rehab - A Poetry Anthology On The Journey To RecoveryEric MaclennanAinda não há avaliações
- SPM English Language Module Set I 2014Documento13 páginasSPM English Language Module Set I 2014Nor Fadzleen100% (7)
- Ch011 EditedDocumento23 páginasCh011 EditedDonny Jinjae Kim-adamsAinda não há avaliações
- Treating Addiction With TunesDocumento10 páginasTreating Addiction With TunesHajrudinAinda não há avaliações
- Physiology of Addiction HandoutDocumento17 páginasPhysiology of Addiction HandoutDawn FarmAinda não há avaliações
- Living Recovery True Stories of Addiction RecoveryDocumento8 páginasLiving Recovery True Stories of Addiction RecoveryIulian MitranAinda não há avaliações
- Words Matter!: Language Statement & Reference GuideDocumento7 páginasWords Matter!: Language Statement & Reference GuideJonas von HoffmannAinda não há avaliações
- Psychiatry Research: NeuroimagingDocumento7 páginasPsychiatry Research: NeuroimagingzzooooeeeeeeAinda não há avaliações
- Nicotine Withdrawal SymptomsDocumento6 páginasNicotine Withdrawal SymptomsNo OneAinda não há avaliações
- Yasmin HurdDocumento41 páginasYasmin HurdNational Press FoundationAinda não há avaliações
- Tatarsky+Marlatt 2010Documento6 páginasTatarsky+Marlatt 2010Iyari LovegoodAinda não há avaliações
- Pima County v. Purdue Parma Et Al. - Complaint (Filed 1.17.19)Documento94 páginasPima County v. Purdue Parma Et Al. - Complaint (Filed 1.17.19)KOLD News 13Ainda não há avaliações
- WEEK 1-8 (24 HRS.) NSTP 1 (Cwts 1) Civic Welfare Training ServiceDocumento19 páginasWEEK 1-8 (24 HRS.) NSTP 1 (Cwts 1) Civic Welfare Training ServiceSheen Hezel MagbanuaAinda não há avaliações
- Seminar Drug AddictionDocumento49 páginasSeminar Drug AddictionJOHN ARBIE TATTAO, RN82% (17)
- Napddr Ddac Info enDocumento27 páginasNapddr Ddac Info ensujeet kumar srivastavaAinda não há avaliações
- ATI Flash Cards 05, Medications Affecting The Nervous SystemDocumento110 páginasATI Flash Cards 05, Medications Affecting The Nervous SystemGiovanni MictilAinda não há avaliações
- Addiction of Chewing Momma by The Residents of Lower Mangga, Tuding, Itogon, Benguet, PhilippinesDocumento22 páginasAddiction of Chewing Momma by The Residents of Lower Mangga, Tuding, Itogon, Benguet, PhilippinesJoel Mangallay100% (1)
- El Proyecto de InglesDocumento3 páginasEl Proyecto de Ingleskim jojoAinda não há avaliações
- 4th FinalsDocumento8 páginas4th Finalsangeline valdez-panis100% (1)
- Module 3 Drug EducationDocumento78 páginasModule 3 Drug EducationLaliene RosalesAinda não há avaliações
- Safa Thesis FinalDocumento12 páginasSafa Thesis FinalSaifi RizwanAinda não há avaliações
- Q2 - Grade 9 - Week 4 - Day 2 - Health - NuestroDocumento4 páginasQ2 - Grade 9 - Week 4 - Day 2 - Health - Nuestrorica may nuestroAinda não há avaliações
- Video Game AddictionDocumento29 páginasVideo Game AddictionNikunj Agrawal0% (1)
- 04 Handout 1 PerdevDocumento2 páginas04 Handout 1 PerdevKing CjAinda não há avaliações
- Be Educated Crystal MethDocumento23 páginasBe Educated Crystal Methapi-374574782% (28)
- Jewish Standard, November 2, 2018Documento60 páginasJewish Standard, November 2, 2018New Jersey Jewish StandardAinda não há avaliações
- The Narcotic Drugs and Psychotropic Substances ActDocumento15 páginasThe Narcotic Drugs and Psychotropic Substances ActPooja MeenaAinda não há avaliações
- Alcohol and DrugsDocumento18 páginasAlcohol and DrugsbeautyAinda não há avaliações
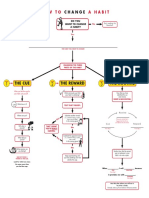
- Flowchart How To Change A Habit PDFDocumento1 páginaFlowchart How To Change A Habit PDFAjit Singh100% (1)