Você também pode gostar
- Skenario: Klarifikasi IstilahDocumento3 páginasSkenario: Klarifikasi IstilahTiara ChairunisaAinda não há avaliações
- Jadwal Jaga Dokter Internsip: KIA UmumDocumento4 páginasJadwal Jaga Dokter Internsip: KIA UmumTiara ChairunisaAinda não há avaliações
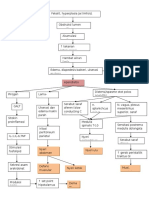
- Pa To GenesisDocumento1 páginaPa To GenesisTiara ChairunisaAinda não há avaliações
- Algo ArrestDocumento2 páginasAlgo ArrestLocomotorica FK UkiAinda não há avaliações
- Snake Bites: SymptomsDocumento2 páginasSnake Bites: SymptomsTiara ChairunisaAinda não há avaliações
- Lec2 Sem7 Year4 EYEwk2 2013 02 09Documento6 páginasLec2 Sem7 Year4 EYEwk2 2013 02 09Tiara ChairunisaAinda não há avaliações
- Higher Algebra - Hall & KnightDocumento593 páginasHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Lap or An 2Documento34 páginasLap or An 2Tiara ChairunisaAinda não há avaliações
- MR SimpleDocumento20 páginasMR SimpleTiara ChairunisaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Sleep Disorder Screening ToolDocumento2 páginasSleep Disorder Screening ToolVivek TiwariAinda não há avaliações
- Soal Efn 1 UtsDocumento3 páginasSoal Efn 1 UtsTri PynAinda não há avaliações
- SOP Akupresur MigrainDocumento20 páginasSOP Akupresur MigrainrachelAinda não há avaliações
- Cancer - GuidelinesDocumento119 páginasCancer - GuidelinesChelleyOllitroAinda não há avaliações
- Infective EndocarditisDocumento68 páginasInfective EndocarditisDr. Rajesh PadhiAinda não há avaliações
- Thyroid Disease Anesthetic ConsiderationsDocumento30 páginasThyroid Disease Anesthetic ConsiderationsmirzaoctaAinda não há avaliações
- Gender Dysphoria & ADHDDocumento21 páginasGender Dysphoria & ADHDAndrew StewartAinda não há avaliações
- Mexican Bed BugDocumento10 páginasMexican Bed BugPatrick Ross Serquiña DulayAinda não há avaliações
- Gerontological Nursing 2021Documento157 páginasGerontological Nursing 2021Andrew Isiah BonifacioAinda não há avaliações
- HistoryandPhysicalExamDocumento105 páginasHistoryandPhysicalExamsilentscream0618Ainda não há avaliações
- Rectal Prolapse: DR Anas Ahmad PGR - Surgical Unit 2 Shalamar Hospital-LahoreDocumento37 páginasRectal Prolapse: DR Anas Ahmad PGR - Surgical Unit 2 Shalamar Hospital-LahoreReshu ThakuriAinda não há avaliações
- Cefuroxime Drug StudyDocumento4 páginasCefuroxime Drug StudyDona Jane BritosAinda não há avaliações
- PSYCH-POST-TESTDocumento27 páginasPSYCH-POST-TESTAdine Jeminah LimonAinda não há avaliações
- Physical Examination of The Critically Injured AthleteDocumento25 páginasPhysical Examination of The Critically Injured Athletebrida.bluesAinda não há avaliações
- Universidad Santiago de CaliDocumento3 páginasUniversidad Santiago de CaliValentina MorenoAinda não há avaliações
- Paclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0Documento7 páginasPaclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0smokkerAinda não há avaliações
- Comparing Ultra-Hypofractionated Proton Versus Photon Therapy in Extremity Soft Tissue SarcomaDocumento10 páginasComparing Ultra-Hypofractionated Proton Versus Photon Therapy in Extremity Soft Tissue SarcomaRaul Matute MartinAinda não há avaliações
- Hemolytic AnemiaDocumento99 páginasHemolytic AnemiaSagar Chandrakant Mhetre100% (3)
- Erbs Palsy PDFDocumento4 páginasErbs Palsy PDFKamran AfzalAinda não há avaliações
- Pathophysiology of CryptorchidismDocumento5 páginasPathophysiology of CryptorchidismAlaiza Aberasturi50% (2)
- Comprehension Activity Story 1: (One Hour Later)Documento2 páginasComprehension Activity Story 1: (One Hour Later)mihai cristinaAinda não há avaliações
- Neurological DiseasesDocumento91 páginasNeurological Diseasesrabia khalidAinda não há avaliações
- PolioDocumento14 páginasPolioapi-31767091450% (2)
- Massage - Pre-Event Massage QuestionnaireDocumento1 páginaMassage - Pre-Event Massage QuestionnaireJerry GAinda não há avaliações
- Delirium: Continuum Lifelong Learning Neurol 2010 16 (2) :120-134Documento15 páginasDelirium: Continuum Lifelong Learning Neurol 2010 16 (2) :120-134Maria Isabel Montañez RestrepoAinda não há avaliações
- Nclex AobyDocumento7 páginasNclex Aobyvienny kayeAinda não há avaliações
- CMT 05210 Internal MedicineDocumento23 páginasCMT 05210 Internal MedicineBashiru SelemaniAinda não há avaliações
- Adapted Study Guide Cellular AdaptationDocumento2 páginasAdapted Study Guide Cellular AdaptationmegAinda não há avaliações
- Nutrition in Intensive Care UnitDocumento21 páginasNutrition in Intensive Care UnitAstri Novia RizqiAinda não há avaliações
- Usos de Bite Blocks PDFDocumento25 páginasUsos de Bite Blocks PDFNatasha RiveraAinda não há avaliações