Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Simple Euler StrutDocumento16 páginasSimple Euler StrutDaniel MabengoAinda não há avaliações
- FEED Deliverable List (Sample) : Project InformationDocumento3 páginasFEED Deliverable List (Sample) : Project Informationamilasri100% (1)
- Standard MissileDocumento2 páginasStandard Missilemadox_3m100% (1)
- MSDS Aradur 2965 PDFDocumento9 páginasMSDS Aradur 2965 PDFkamalnandreAinda não há avaliações
- Zeolites and Ordered Porous Solids - Fundamentals and ApplicationsDocumento376 páginasZeolites and Ordered Porous Solids - Fundamentals and ApplicationsHenrique Souza100% (1)
- Oral PigmentedDocumento16 páginasOral PigmentedZulfahmi NurdinAinda não há avaliações
- SonicFill Handpiece Instructions For UseDocumento58 páginasSonicFill Handpiece Instructions For UseZulfahmi NurdinAinda não há avaliações
- 4gauging GTXDocumento1 página4gauging GTXZulfahmi NurdinAinda não há avaliações
- Brochure-Gc Fuji ViiDocumento16 páginasBrochure-Gc Fuji ViiZulfahmi NurdinAinda não há avaliações
- SonicFill 2 Technique GuideDocumento1 páginaSonicFill 2 Technique GuideZulfahmi NurdinAinda não há avaliações
- Effect of Refrigeration On Bond Strength of Self-Etching Adhesive SystemsDocumento5 páginasEffect of Refrigeration On Bond Strength of Self-Etching Adhesive SystemsZulfahmi NurdinAinda não há avaliações
- Dentj 39 2 04Documento4 páginasDentj 39 2 04Zulfahmi NurdinAinda não há avaliações
- Indications and Case Series of Intentional Replantation of TeethDocumento8 páginasIndications and Case Series of Intentional Replantation of TeethZulfahmi NurdinAinda não há avaliações
- Ludwig's Angina - An Emergency: A Case Report With Literature ReviewDocumento7 páginasLudwig's Angina - An Emergency: A Case Report With Literature ReviewZulfahmi NurdinAinda não há avaliações
- Ellagic Acid Information & ReferencesDocumento6 páginasEllagic Acid Information & ReferencesZulfahmi NurdinAinda não há avaliações
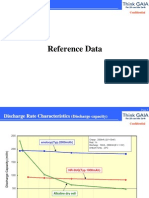
- Discharge Characteristics 3UQDocumento5 páginasDischarge Characteristics 3UQZulfahmi NurdinAinda não há avaliações
- Cariesactivitytests 090722115427 Phpapp01Documento14 páginasCariesactivitytests 090722115427 Phpapp01Zulfahmi NurdinAinda não há avaliações
- Relay Identification: Example CDG31FF002SACHDocumento5 páginasRelay Identification: Example CDG31FF002SACHRohit RanaAinda não há avaliações
- 5-2 Sem2 Phys ExamDocumento7 páginas5-2 Sem2 Phys ExamNayLinAinda não há avaliações
- Wolfi Landstreicher - Willful Disobedience - Number 3Documento32 páginasWolfi Landstreicher - Willful Disobedience - Number 3populaererAinda não há avaliações
- AsasDocumento2 páginasAsasbuntu2003Ainda não há avaliações
- C.4. Quiz Conservation of BiodiversityDocumento2 páginasC.4. Quiz Conservation of Biodiversitylaura pongutaAinda não há avaliações
- Portland PortDocumento18 páginasPortland PortAnonymous Lx3jPjHAVLAinda não há avaliações
- Unit-4 - Hypothesis TestingDocumento24 páginasUnit-4 - Hypothesis TestingMANTHAN JADHAVAinda não há avaliações
- Cleavage in MammalsDocumento51 páginasCleavage in MammalsIrfan Azram100% (4)
- Antena Kathrein 742266 PDFDocumento2 páginasAntena Kathrein 742266 PDFcesarbayonaAinda não há avaliações
- Seismic Retrofitting2.0 BY PRIYANSHUDocumento30 páginasSeismic Retrofitting2.0 BY PRIYANSHUPriyanshu VarshneyAinda não há avaliações
- Lesson Plan 1 - Agriculture in Your LifeDocumento6 páginasLesson Plan 1 - Agriculture in Your Lifeapi-235918896Ainda não há avaliações
- Energy and FluctuationDocumento10 páginasEnergy and Fluctuationwalid Ait MazouzAinda não há avaliações
- Prepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentDocumento11 páginasPrepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentwaqasAinda não há avaliações
- Anritsu Metal Detection GuideDocumento32 páginasAnritsu Metal Detection GuideJesus Roberto De La Vega GermanAinda não há avaliações
- TNB Ar2011Documento334 páginasTNB Ar2011Duncan LeeAinda não há avaliações
- Gayatri Mantras of Several GodDocumento10 páginasGayatri Mantras of Several GodAnup KashyapAinda não há avaliações
- Fighting The Sixth Mass ExtinctionDocumento25 páginasFighting The Sixth Mass ExtinctionRichard J. MarksAinda não há avaliações
- Power System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustDocumento10 páginasPower System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustShahab SaqibAinda não há avaliações
- F115a'12 Fl115a'12: (68VB) (68WB)Documento96 páginasF115a'12 Fl115a'12: (68VB) (68WB)AlexDiazAinda não há avaliações
- Bugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54Documento9.715 páginasBugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54João Carlos Pereira ChoinasAinda não há avaliações
- Iso 3932 1976Documento8 páginasIso 3932 1976NaveedAinda não há avaliações
- Favino Circulation of Scientific Knowledge AcroDocumento8 páginasFavino Circulation of Scientific Knowledge AcroPeter FryAinda não há avaliações
- ASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFDocumento5 páginasASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFАртем ТитовAinda não há avaliações
- Ambitious Academy Lahore: Annual Revision Test SystemDocumento2 páginasAmbitious Academy Lahore: Annual Revision Test SystemAmir HabibAinda não há avaliações
- Zen Intro To Buddhism & Practice of ZazenDocumento33 páginasZen Intro To Buddhism & Practice of ZazendudcomeonAinda não há avaliações