Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Case Study On ThyroidectomyDocumento45 páginasCase Study On Thyroidectomyjamallecar82% (11)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Iodine - The Universal and Holistic Super Mineral - Dr. Gabriel CousensDocumento32 páginasIodine - The Universal and Holistic Super Mineral - Dr. Gabriel CousensJ.J.100% (7)
- Quiz EndocrineDocumento84 páginasQuiz EndocrineMedShare92% (12)
- HyperthyroidismDocumento18 páginasHyperthyroidismWahyuni FatmonaAinda não há avaliações
- A Study On Thyroid Function Test in Children With Nephrotic SyndromeDocumento3 páginasA Study On Thyroid Function Test in Children With Nephrotic Syndromeamallia_nsAinda não há avaliações
- TRIK 1 - 21 TOEFL OnlineDocumento165 páginasTRIK 1 - 21 TOEFL OnlineIsmita HadiyantiAinda não há avaliações
- Unrefined Salt-Iodine Lecture-M Schachter MD ACAM 10-25-10 8-45 PM Reviewed 9-24-18Documento128 páginasUnrefined Salt-Iodine Lecture-M Schachter MD ACAM 10-25-10 8-45 PM Reviewed 9-24-18kobreedingAinda não há avaliações
- (Pediaii) 013 Pediatric Endocrine DisordersDocumento29 páginas(Pediaii) 013 Pediatric Endocrine DisordersdoktoraronaAinda não há avaliações
- Thyroid Colloid Nodular GoiterDocumento23 páginasThyroid Colloid Nodular Goitervahn025Ainda não há avaliações
- Activating AutophagyDocumento59 páginasActivating Autophagynomedacerniauskaite6600100% (19)
- Chapter 49 - Thyroid and Parathyroid DisordersDocumento7 páginasChapter 49 - Thyroid and Parathyroid DisordersStacey100% (1)
- Johanna Jane H. Macasero - Endocrine System TranscriptDocumento13 páginasJohanna Jane H. Macasero - Endocrine System TranscriptJohanna MacaseroAinda não há avaliações
- Thyroid Storm: Karthik Balachandran Karthik2k2Documento52 páginasThyroid Storm: Karthik Balachandran Karthik2k2Dr Karthik Balachandran, EndocrinologyAinda não há avaliações
- 2nd Journal - Andre Parmonangan Panjaitan - 013Documento7 páginas2nd Journal - Andre Parmonangan Panjaitan - 013Andre Parmonangan PanjaitanAinda não há avaliações
- MCQs For LaboratoryDocumento42 páginasMCQs For LaboratorySami Khan87% (68)
- Benign Diseases of ThyroidDocumento70 páginasBenign Diseases of ThyroidMounica MekalaAinda não há avaliações
- Endocrine - FRCEM SuccessDocumento110 páginasEndocrine - FRCEM SuccessskAinda não há avaliações
- MB CHB: Faculty of MedicineDocumento45 páginasMB CHB: Faculty of MedicineMuhammad SadiqAinda não há avaliações
- Drug Cards EndoDocumento12 páginasDrug Cards EndoChristine Schroeder100% (1)
- End of Report : Dr. Shashidhar., MD (Path) (Lab Technician) Consultant PathologistDocumento10 páginasEnd of Report : Dr. Shashidhar., MD (Path) (Lab Technician) Consultant PathologistAnonymous Jm5SLbvAinda não há avaliações
- Dental Conditions in Patients With Bipolar Disorder On Long-Term Lithium Maintenance TherapyDocumento4 páginasDental Conditions in Patients With Bipolar Disorder On Long-Term Lithium Maintenance TherapyCosminAinda não há avaliações
- Exercise 4: Endocrine System Physiology: Activity 1: Metabolism and Thyroid Hormone Lab ReportDocumento7 páginasExercise 4: Endocrine System Physiology: Activity 1: Metabolism and Thyroid Hormone Lab ReportAlexandru BurdeniucAinda não há avaliações
- Fisiologi Hormon TiroidDocumento54 páginasFisiologi Hormon Tiroidaan SyamhaAinda não há avaliações
- L34 - MR - Nilesh Yadav - Kota CC 6 RAY-99/100, Bajrang Nagar Main Road, Near Bright Land School, Kota-324001Documento11 páginasL34 - MR - Nilesh Yadav - Kota CC 6 RAY-99/100, Bajrang Nagar Main Road, Near Bright Land School, Kota-324001Shivam MittalAinda não há avaliações
- Pharmacology of ThyroidDocumento32 páginasPharmacology of Thyroidbrigita charvioAinda não há avaliações
- Pediatric Normal Laboratory ValuesDocumento15 páginasPediatric Normal Laboratory ValuesAkhmad Dani AwaludinAinda não há avaliações
- Apbio 45 LectoutDocumento15 páginasApbio 45 LectoutSimone Alexis GuinocorAinda não há avaliações
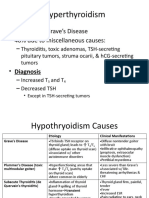
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocumento6 páginasHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.Ainda não há avaliações
- Topic 1 Endocrine SystemDocumento140 páginasTopic 1 Endocrine SystemmasdfgAinda não há avaliações
- Polly Hattemer Book 4 HormonesDocumento80 páginasPolly Hattemer Book 4 Hormonessusilorini100% (2)