Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Divorce Bill in The PhilippinesDocumento19 páginasDivorce Bill in The PhilippinesNeiqui Aubrey Antaran CañeteAinda não há avaliações
- Tech - Speed Strength Endurance in 400Documento7 páginasTech - Speed Strength Endurance in 400jeyAinda não há avaliações
- 4ps QuestionnaireDocumento3 páginas4ps QuestionnaireFlorante De Leon67% (3)
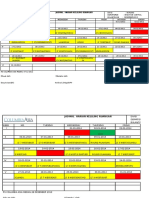
- Jadwal Keliling Hariaan 2014Documento38 páginasJadwal Keliling Hariaan 2014Desy ArisandiAinda não há avaliações
- Training Tanggap DaruratDocumento2 páginasTraining Tanggap DaruratDesy ArisandiAinda não há avaliações
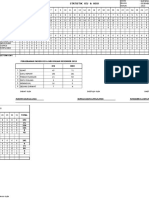
- Statistik 2014Documento21 páginasStatistik 2014Desy ArisandiAinda não há avaliações
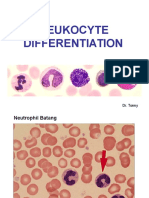
- Leukocyte Differentiation GuideDocumento16 páginasLeukocyte Differentiation GuideDesy ArisandiAinda não há avaliações
- Leukocyte Differentiation GuideDocumento16 páginasLeukocyte Differentiation GuideDesy ArisandiAinda não há avaliações
- Ibu Onne Myrna - Infection Control 2012Documento27 páginasIbu Onne Myrna - Infection Control 2012Desy ArisandiAinda não há avaliações
- New Dll-Math Week 4-1Documento3 páginasNew Dll-Math Week 4-1AstroAinda não há avaliações
- Equivalent Representations, Useful Forms, Functions of Square MatricesDocumento57 páginasEquivalent Representations, Useful Forms, Functions of Square MatricesWiccy IhenaAinda não há avaliações
- Agganna Sutta - Theory of KingshipDocumento8 páginasAgganna Sutta - Theory of KingshipTanya ChopraAinda não há avaliações
- Geppetto's Wish Comes True: Pinocchio Becomes a Real BoyDocumento1 páginaGeppetto's Wish Comes True: Pinocchio Becomes a Real BoyDonzAinda não há avaliações
- Technical and Cost Model For Slipway DevelopmentDocumento36 páginasTechnical and Cost Model For Slipway DevelopmentshahjadaAinda não há avaliações
- Mythical Origins of The Hungarian Medieval LegislationDocumento8 páginasMythical Origins of The Hungarian Medieval LegislationLucas LixaAinda não há avaliações
- Reporter Matt Rudd Goes On An Extraordinary Plane RideDocumento2 páginasReporter Matt Rudd Goes On An Extraordinary Plane RideHAnhh TrầnnAinda não há avaliações
- Dreams PDFDocumento8 páginasDreams PDFapi-266967947Ainda não há avaliações
- THE QUALITY OF LITERARY ENGLISH VIETNAMESE TRANSLATIONS TODAY. LƯỜNG THỊ THÚY.QH.1.EDocumento64 páginasTHE QUALITY OF LITERARY ENGLISH VIETNAMESE TRANSLATIONS TODAY. LƯỜNG THỊ THÚY.QH.1.EKavic100% (2)
- Explain Mod 4Documento20 páginasExplain Mod 4Gab IgnacioAinda não há avaliações
- Flyposting OrdinanceDocumento2 páginasFlyposting OrdinanceJunil LagardeAinda não há avaliações
- Creating A Seasonal Greeting Card RubricDocumento3 páginasCreating A Seasonal Greeting Card Rubricapi-244997750Ainda não há avaliações
- Data Acquisition Systems Communicate With Microprocessors Over 4 WiresDocumento2 páginasData Acquisition Systems Communicate With Microprocessors Over 4 WiresAnonymous Y6EW7E1Gb3Ainda não há avaliações
- 2012 C R I M I N A L L A W 1 Reviewer Wordpresscom 5a237cee1723dd6eef7c227dDocumento15 páginas2012 C R I M I N A L L A W 1 Reviewer Wordpresscom 5a237cee1723dd6eef7c227dSan PedroAinda não há avaliações
- Concept AttainmentDocumento1 páginaConcept Attainmentapi-189549713Ainda não há avaliações
- Activity SheetmagnetismDocumento8 páginasActivity SheetmagnetismLey F. Fajutagana100% (1)
- Development Through The Lifespan Test 1Documento3 páginasDevelopment Through The Lifespan Test 1Alexandra CastroAinda não há avaliações
- LESSON 1.1.2 - Online PlatformsDocumento5 páginasLESSON 1.1.2 - Online PlatformsAndree Laxamana100% (1)
- Comparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 YearsDocumento4 páginasComparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 Yearsmanjula dangeAinda não há avaliações
- Car For Sale: A. Here Are Some More Car Ads. Read Them and Complete The Answers BelowDocumento5 páginasCar For Sale: A. Here Are Some More Car Ads. Read Them and Complete The Answers BelowCésar Cordova DíazAinda não há avaliações
- Irish Chapter 6 Causes of DeathDocumento8 páginasIrish Chapter 6 Causes of DeathIrish AlonzoAinda não há avaliações
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDocumento15 páginasCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarAinda não há avaliações
- Fourth Edition Hungarian WordlistDocumento12 páginasFourth Edition Hungarian WordlistMarton HorvathAinda não há avaliações
- Maintain Records and Bond EmployeesDocumento5 páginasMaintain Records and Bond EmployeesAngel Frankie RamosAinda não há avaliações
- Solución: R T β T R (T) = 1000 Ω ΩDocumento6 páginasSolución: R T β T R (T) = 1000 Ω ΩDuvan BayonaAinda não há avaliações
- Princes of the Apocalypse Locations IndexDocumento2 páginasPrinces of the Apocalypse Locations IndexPedroManzelaDuarteAinda não há avaliações
- Karakteristik Morfologik Kambing Spesifik Lokal Di Kabupaten Samosir Sumatera UtaraDocumento6 páginasKarakteristik Morfologik Kambing Spesifik Lokal Di Kabupaten Samosir Sumatera UtaraOlivia SimanungkalitAinda não há avaliações