Você também pode gostar
- Diy Home Made 6w Led BulbDocumento7 páginasDiy Home Made 6w Led BulbjnaguAinda não há avaliações
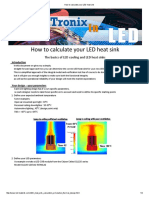
- How to calculate your LED heat sinkDocumento4 páginasHow to calculate your LED heat sinkjnaguAinda não há avaliações
- Low Cost 150 Watt Amplifier CircuitDocumento3 páginasLow Cost 150 Watt Amplifier CircuitjnaguAinda não há avaliações
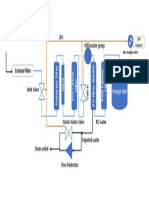
- Filter ProcessDocumento1 páginaFilter ProcessjnaguAinda não há avaliações
- 2.3.4 The Ball Shall Be of A Brand and Type Currently Approved by The ITTFDocumento2 páginas2.3.4 The Ball Shall Be of A Brand and Type Currently Approved by The ITTFjnaguAinda não há avaliações
- Benefits of Cardamom and TurmericDocumento11 páginasBenefits of Cardamom and TurmericjnaguAinda não há avaliações
- White Paper Next Gen End Point ProtectionDocumento15 páginasWhite Paper Next Gen End Point ProtectionjnaguAinda não há avaliações
- Comparison of CPU performance at different clock speedsDocumento1 páginaComparison of CPU performance at different clock speedsjnaguAinda não há avaliações
- Ba 33301306Documento6 páginasBa 33301306Shakeel RanaAinda não há avaliações
- Comparison of CPU performance at different clock speedsDocumento1 páginaComparison of CPU performance at different clock speedsjnaguAinda não há avaliações
- Diy Home Made 6w Led BulbDocumento7 páginasDiy Home Made 6w Led BulbjnaguAinda não há avaliações
- Keerai BenefitsDocumento3 páginasKeerai BenefitsjnaguAinda não há avaliações
- Prospectus New India Floater Medi ClaimDocumento17 páginasProspectus New India Floater Medi ClaimPriyank GuptaAinda não há avaliações
- Price ListDocumento22 páginasPrice ListjnaguAinda não há avaliações
- Benefits of Cardamom and TurmericDocumento11 páginasBenefits of Cardamom and TurmericjnaguAinda não há avaliações
- DevOps Tutorial - Introduction To DevOps - EdurekaDocumento10 páginasDevOps Tutorial - Introduction To DevOps - EdurekajnaguAinda não há avaliações
- OnlineecDocumento131 páginasOnlineecjnaguAinda não há avaliações
- Tennis: A guide to the rules and gameplay of this popular racquet sportDocumento3 páginasTennis: A guide to the rules and gameplay of this popular racquet sportjnaguAinda não há avaliações
- Filter ProcessDocumento1 páginaFilter ProcessjnaguAinda não há avaliações
- Tennis: A guide to the rules and gameplay of this popular racquet sportDocumento3 páginasTennis: A guide to the rules and gameplay of this popular racquet sportjnaguAinda não há avaliações
- Kodai - Naidupuram Srivijayalakshmi NagarDocumento1 páginaKodai - Naidupuram Srivijayalakshmi NagarjnaguAinda não há avaliações
- Mudakathan Keerai Benefits for Joint PainDocumento3 páginasMudakathan Keerai Benefits for Joint PainjnaguAinda não há avaliações
- Tennis OriginDocumento3 páginasTennis OriginjnaguAinda não há avaliações
- Follow These Steps (1 To 9) To Plan Your TripDocumento3 páginasFollow These Steps (1 To 9) To Plan Your TripjnaguAinda não há avaliações
- Protecting Your House From Termites: Environmental Health GuideDocumento6 páginasProtecting Your House From Termites: Environmental Health GuidejnaguAinda não há avaliações
- Ds 5600 ApplianceDocumento4 páginasDs 5600 ApplianceMatthew MathewsAinda não há avaliações
- Tennis OriginDocumento3 páginasTennis OriginjnaguAinda não há avaliações
- Keerai BenefitsDocumento3 páginasKeerai BenefitsjnaguAinda não há avaliações
- ISMS Consultancy For JPKN - Project Kickoff MeetingDocumento23 páginasISMS Consultancy For JPKN - Project Kickoff Meetingjnagu50% (2)
- BSI Standard 100-1Documento38 páginasBSI Standard 100-1Carlo CafieroAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Madurai Corporation Contempt CaseDocumento6 páginasMadurai Corporation Contempt Caseforpublic 2011100% (1)
- Biological Basis of BehaviourDocumento6 páginasBiological Basis of BehaviourRichard ManuelAinda não há avaliações
- 6529XXXXXXXXXX34 01-05-2023 UnlockedDocumento2 páginas6529XXXXXXXXXX34 01-05-2023 UnlockedSath KAinda não há avaliações
- Poultry Farm Business PlanDocumento4 páginasPoultry Farm Business PlanAbdul Basit Bazaz100% (1)
- TBM220Documento12 páginasTBM220ErikoAinda não há avaliações
- Upt SMP Negeri 5 Pasarkemis: Dinas PendidikanDocumento2 páginasUpt SMP Negeri 5 Pasarkemis: Dinas Pendidikanara ibagaztaAinda não há avaliações
- Ochem Lab Research PaperDocumento2 páginasOchem Lab Research Papermohamed abukarAinda não há avaliações
- Casa 212 Inst-A5Documento8 páginasCasa 212 Inst-A5handokoAinda não há avaliações
- I Saw The Light - Stan Slack BanjoDocumento2 páginasI Saw The Light - Stan Slack BanjoEAinda não há avaliações
- Nighshift Magazine - December 2011Documento24 páginasNighshift Magazine - December 2011wpl955gAinda não há avaliações
- Mvusd 2014-2015 CalendarDocumento1 páginaMvusd 2014-2015 Calendarapi-255097501Ainda não há avaliações
- Mid Term Date Sheet - pq0NsApDocumento2 páginasMid Term Date Sheet - pq0NsApSahil HansAinda não há avaliações
- GSPpermitDocumento2 páginasGSPpermitjoveyAinda não há avaliações
- Celular LG CodesDocumento6 páginasCelular LG CodesGeorgeAinda não há avaliações
- Economy India (Bain Report)Documento103 páginasEconomy India (Bain Report)Yogesh GuttaAinda não há avaliações
- Visa Application Form SummaryDocumento1 páginaVisa Application Form Summaryshouaib hussainAinda não há avaliações
- Ejercicios de Presente Simple y Presente Continuo PDFDocumento2 páginasEjercicios de Presente Simple y Presente Continuo PDFAlfonso DíezAinda não há avaliações
- Removal of Sulfide and COD From A Crude Oil Wastewater Model by Aluminum and Iron ElectrocoagulationDocumento4 páginasRemoval of Sulfide and COD From A Crude Oil Wastewater Model by Aluminum and Iron ElectrocoagulationEhab DheyaaAinda não há avaliações
- Reading Sample Test 1 Answer Key Part A B CDocumento4 páginasReading Sample Test 1 Answer Key Part A B Cyiğit ezenAinda não há avaliações
- July-November 2021: CH 429 Petroleum and Petrochemicals (3-0-0-6)Documento33 páginasJuly-November 2021: CH 429 Petroleum and Petrochemicals (3-0-0-6)shubhamAinda não há avaliações
- Tour Report - Quality Control and Improvement of Glass Industries LimitedDocumento30 páginasTour Report - Quality Control and Improvement of Glass Industries LimitedCryptic Sufi0% (1)
- In-Circuit and In-Application Programming of The 89C51Rx+/Rx2/66x MicrocontrollersDocumento17 páginasIn-Circuit and In-Application Programming of The 89C51Rx+/Rx2/66x Microcontrollersv1swaroopAinda não há avaliações
- Building Planning: Dr. Anantha Singh T. SDocumento20 páginasBuilding Planning: Dr. Anantha Singh T. SUtsav modhAinda não há avaliações
- Unity 400Documento61 páginasUnity 400Aitonix ScanAinda não há avaliações
- Makkah Train Network ProjectDocumento3 páginasMakkah Train Network ProjectSTP DesignAinda não há avaliações
- Non FictionDocumento5 páginasNon FictionSlick IncubatorsAinda não há avaliações
- Template How-To: Purpose of This TemplateDocumento5 páginasTemplate How-To: Purpose of This TemplateLouis TrầnAinda não há avaliações
- Guide To Indian ManuscriptsDocumento86 páginasGuide To Indian Manuscriptsshahrad87Ainda não há avaliações
- Electrical Safety Devices at Home: Science 8Documento5 páginasElectrical Safety Devices at Home: Science 8John Mark PrestozaAinda não há avaliações
- Dating - Find Love with the Top Free Dating SiteDocumento1 páginaDating - Find Love with the Top Free Dating SiteSss NmmAinda não há avaliações