Você também pode gostar
- Erin Condren Project - StickersDocumento14 páginasErin Condren Project - StickersSiska FriedmanAinda não há avaliações
- B - Yonanda Adi (Stroke)Documento10 páginasB - Yonanda Adi (Stroke)Siska FriedmanAinda não há avaliações
- Erin Condren Project - StickersDocumento14 páginasErin Condren Project - StickersSiska FriedmanAinda não há avaliações
- Can You Help Fairies Find Their HomeDocumento1 páginaCan You Help Fairies Find Their HomeSiska FriedmanAinda não há avaliações
- Lidarwati Zega Jog W7lupv HLP Flight OriginatingDocumento2 páginasLidarwati Zega Jog W7lupv HLP Flight OriginatingSiska FriedmanAinda não há avaliações
- Pre EclampsiaDocumento15 páginasPre EclampsiaSiska FriedmanAinda não há avaliações
- D - Rochmanita Safitri (Skoliosis)Documento59 páginasD - Rochmanita Safitri (Skoliosis)Siska FriedmanAinda não há avaliações
- DTSCH Arztebl Int-110-0227Documento10 páginasDTSCH Arztebl Int-110-0227Siska FriedmanAinda não há avaliações
- D - Nurain Amirah (Efusi Pleura Ec Adeno CA)Documento17 páginasD - Nurain Amirah (Efusi Pleura Ec Adeno CA)Siska FriedmanAinda não há avaliações
- D - Dayang Norazlia (Calcaneal Spur)Documento14 páginasD - Dayang Norazlia (Calcaneal Spur)Siska FriedmanAinda não há avaliações
- A - Annalisya-Salter HarrisDocumento3 páginasA - Annalisya-Salter HarrisSiska FriedmanAinda não há avaliações
- Diagnosis and Management of Ectopic PregnancyDocumento7 páginasDiagnosis and Management of Ectopic PregnancyKevin Mora BañosAinda não há avaliações
- C - Kavinan Subramaniam - Heart FailureDocumento5 páginasC - Kavinan Subramaniam - Heart FailureSiska FriedmanAinda não há avaliações
- Hyperemesis GravidarumDocumento12 páginasHyperemesis GravidarumSiska FriedmanAinda não há avaliações
- Bacterial VaginosisDocumento6 páginasBacterial VaginosisSiska FriedmanAinda não há avaliações
- FigureDocumento1 páginaFigureSiska FriedmanAinda não há avaliações
- Induction of LabourDocumento26 páginasInduction of LabourAracely NarváezAinda não há avaliações
- G GDMDocumento38 páginasG GDMSiska FriedmanAinda não há avaliações
- Ectopic PregnancyDocumento3 páginasEctopic PregnancySiska FriedmanAinda não há avaliações
- Figo SteroidDocumento14 páginasFigo SteroidDedy Chandra HariyonoAinda não há avaliações
- G VbacDocumento16 páginasG VbacSiska FriedmanAinda não há avaliações
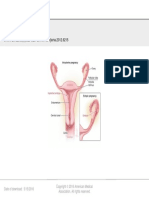
- From: Ectopic Pregnancy: JAMA. 2012 308 (8) :829-829. Doi:10.1001/jama.2012.6215Documento1 páginaFrom: Ectopic Pregnancy: JAMA. 2012 308 (8) :829-829. Doi:10.1001/jama.2012.6215Siska FriedmanAinda não há avaliações
- Figo SteroidDocumento14 páginasFigo SteroidDedy Chandra HariyonoAinda não há avaliações
- Ectopic Pregnancy JournalDocumento3 páginasEctopic Pregnancy JournalSiska FriedmanAinda não há avaliações
- Investigations and Treatments of Recurrent Pregnancy LossDocumento19 páginasInvestigations and Treatments of Recurrent Pregnancy LossSiska FriedmanAinda não há avaliações
- Fakultas Kedokteran Universitas Lampung: Closed Fracture 1/3 Middle Femur DextraDocumento7 páginasFakultas Kedokteran Universitas Lampung: Closed Fracture 1/3 Middle Femur DextraVic Fuentes ScremoAinda não há avaliações
- Plant Start Up Timeline - 24 Aug 09 - Rev 1Documento1 páginaPlant Start Up Timeline - 24 Aug 09 - Rev 1Siska FriedmanAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Solomon On Sex - Avoiding Marital Disaster: February 12, 2012Documento14 páginasSolomon On Sex - Avoiding Marital Disaster: February 12, 2012baimareanAinda não há avaliações
- Most Important One Liner Questions and Answers May 2022Documento15 páginasMost Important One Liner Questions and Answers May 2022pradeepAinda não há avaliações
- PDFDocumento8 páginasPDFDocAinda não há avaliações
- Lab Centre of Pressure Ecw341Documento4 páginasLab Centre of Pressure Ecw341danialAinda não há avaliações
- Calabano Clinical Bacteriology Exercise 1Documento5 páginasCalabano Clinical Bacteriology Exercise 1MarkJasperCalabanoAinda não há avaliações
- Disa Match: A Match You Can Count OnDocumento8 páginasDisa Match: A Match You Can Count OngAinda não há avaliações
- Logistics Operation PlanningDocumento25 páginasLogistics Operation PlanningLeonard AntoniusAinda não há avaliações
- Scientific American Psychology 2nd Edition Licht Test BankDocumento44 páginasScientific American Psychology 2nd Edition Licht Test Bankpurelychittra3ae3100% (24)
- Refrigeration Engineer Quick ReferenceDocumento2 páginasRefrigeration Engineer Quick ReferenceventilationAinda não há avaliações
- Mid-Year Examination, 2023 Science Year 7 1 HourDocumento23 páginasMid-Year Examination, 2023 Science Year 7 1 HourAl-Hafiz Bin SajahanAinda não há avaliações
- General Anaesthesia MCQsDocumento5 páginasGeneral Anaesthesia MCQsWasi Khan100% (3)
- Assignment On Cholera: Submitted ToDocumento17 páginasAssignment On Cholera: Submitted ToEhesanulHaqueSaifAinda não há avaliações
- Faujifood Pakistan PortfolioDocumento21 páginasFaujifood Pakistan PortfolioPradeep AbeynayakeAinda não há avaliações
- Varaah KavachDocumento7 páginasVaraah KavachBalagei Nagarajan100% (1)
- Ac 521 007Documento10 páginasAc 521 007JacquesAinda não há avaliações
- Study of Mosquito Larvicidal Effects of (Bitter Gourd) Extracts As NanopowderDocumento3 páginasStudy of Mosquito Larvicidal Effects of (Bitter Gourd) Extracts As NanopowderAnonymous AkoAinda não há avaliações
- VlsiDocumento79 páginasVlsimdhuq1Ainda não há avaliações
- Neuromuscular Diseases. ALSDocumento7 páginasNeuromuscular Diseases. ALSjalan_zAinda não há avaliações
- Working at Heights GuidelineDocumento15 páginasWorking at Heights Guidelinechanks498Ainda não há avaliações
- Fatigue Consideration in DesignDocumento3 páginasFatigue Consideration in DesigngouthamAinda não há avaliações
- FENA-01 - 11 - 21 - Ethernet Adapter - User's Manual - Rev BDocumento388 páginasFENA-01 - 11 - 21 - Ethernet Adapter - User's Manual - Rev BQUOC LEAinda não há avaliações
- Monthly Exam Part I Aurora English Course 1 (KD 1, KD2, PKD3)Documento20 páginasMonthly Exam Part I Aurora English Course 1 (KD 1, KD2, PKD3)winda septiaraAinda não há avaliações
- DiodeDocumento3 páginasDiodeManishAinda não há avaliações
- Tutorial 2Documento2 páginasTutorial 2Adam HakimiAinda não há avaliações
- Microscope MaintenanceDocumento2 páginasMicroscope MaintenanceCharlyn KeithAinda não há avaliações
- Scuba Diving - Technical Terms MK IDocumento107 páginasScuba Diving - Technical Terms MK IJoachim MikkelsenAinda não há avaliações
- 14 WosDocumento6 páginas14 WosATUL KURZEKARAinda não há avaliações
- In Truth To Mollusca According To New Studies by J RutherfordDocumento4 páginasIn Truth To Mollusca According To New Studies by J RutherfordbalaiAinda não há avaliações
- High Performance Dialysis GuideDocumento28 páginasHigh Performance Dialysis GuideRoxana ElenaAinda não há avaliações
- Magneto-Convective Non-Newtonian Nanofluid With Momentum and Temperature Dependent Slip Flow From A Permeable Stretching Sheet With Porous Medium and Chemical ReactionDocumento18 páginasMagneto-Convective Non-Newtonian Nanofluid With Momentum and Temperature Dependent Slip Flow From A Permeable Stretching Sheet With Porous Medium and Chemical ReactionIOSRjournalAinda não há avaliações