Você também pode gostar
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualNo EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualNota: 4.5 de 5 estrelas4.5/5 (2)
- Implant ResearchDocumento8 páginasImplant ResearchFBI LUC1FeRAinda não há avaliações
- Treatment Planning Single Maxillary Anterior Implants for DentistsNo EverandTreatment Planning Single Maxillary Anterior Implants for DentistsAinda não há avaliações
- Clinical Maxillary Sinus Elevation SurgeryNo EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoAinda não há avaliações
- Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsNo EverandSupra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsNota: 5 de 5 estrelas5/5 (1)
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionNo EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionNota: 4 de 5 estrelas4/5 (1)
- Risk Management Oral SurgeryDocumento7 páginasRisk Management Oral SurgerymohsinosmaanAinda não há avaliações
- Bone Ring 3Documento4 páginasBone Ring 3Pradusha RevuruAinda não há avaliações
- Jung 2018Documento11 páginasJung 2018Sebastien MelloulAinda não há avaliações
- Implant-Related Complications and FailuresDocumento91 páginasImplant-Related Complications and FailuresSaman MohammadzadehAinda não há avaliações
- Caldwell TechniqueDocumento4 páginasCaldwell TechniqueNurul RamadhantyAinda não há avaliações
- Controversiesin Anesthesiafororaland Maxillofacialsurgery: Brett J. King,, Adam LevineDocumento9 páginasControversiesin Anesthesiafororaland Maxillofacialsurgery: Brett J. King,, Adam LevineAB MISHRAAinda não há avaliações
- Computeinr Aided Bypass of The Inferior Alveolar NerveDocumento22 páginasComputeinr Aided Bypass of The Inferior Alveolar NerveRhea OngAinda não há avaliações
- 9 Example Thesis For SOP 2014-02-10Documento31 páginas9 Example Thesis For SOP 2014-02-10phileasfoggscribAinda não há avaliações
- Adjuncts For Care of The Surgical Patient Atlas of The Oral and Maxillofacial Surgery ClinicsDocumento71 páginasAdjuncts For Care of The Surgical Patient Atlas of The Oral and Maxillofacial Surgery Clinics嘉妮Ainda não há avaliações
- 5 Steps To A Successful Dental PracticeDocumento22 páginas5 Steps To A Successful Dental PracticeVasile FlorinAinda não há avaliações
- Wang 2021 Imagenologíaen CBMFDocumento21 páginasWang 2021 Imagenologíaen CBMFRocio CacñahuarayAinda não há avaliações
- Zygomatic Implants PDFDocumento18 páginasZygomatic Implants PDFgirl33Ainda não há avaliações
- Implant Surgical AnatomyDocumento14 páginasImplant Surgical AnatomyKo YotoAinda não há avaliações
- Advances in Extraction TechniquesDocumento13 páginasAdvances in Extraction TechniquesashajangamAinda não há avaliações
- Wisdom TeethDocumento3 páginasWisdom TeethPreetam PatnalaAinda não há avaliações
- CC3 Group1 Consensus Stat... EmentsDocumento3 páginasCC3 Group1 Consensus Stat... Ementseveliiiin100% (1)
- Chapter 6 Midi Implant ProcedureDocumento9 páginasChapter 6 Midi Implant Procedurezeus_1949Ainda não há avaliações
- 2015 Kin JIACD - Sticky Bone - Sohn Et Al PDFDocumento20 páginas2015 Kin JIACD - Sticky Bone - Sohn Et Al PDFOscar CabreraAinda não há avaliações
- PLICACIONESDocumento19 páginasPLICACIONESGuillermo RiosAinda não há avaliações
- Misch Seminar Final 6-4-12Documento2 páginasMisch Seminar Final 6-4-12florin013Ainda não há avaliações
- Essentials of Orthognathic Surgery, 2nd Edition: Book ReviewsDocumento1 páginaEssentials of Orthognathic Surgery, 2nd Edition: Book ReviewsPae Anusorn AmtanonAinda não há avaliações
- Case Selection in Dental Implant TherapyDocumento4 páginasCase Selection in Dental Implant Therapymichealraj rousseauAinda não há avaliações
- The Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingDocumento13 páginasThe Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingMikeunoeAinda não há avaliações
- Use of Implants in The Pterygoid Region For Prosthodontic TreatmentDocumento4 páginasUse of Implants in The Pterygoid Region For Prosthodontic TreatmentSidhartha KumarAinda não há avaliações
- Ebook Wisdom Teeth RDocumento3 páginasEbook Wisdom Teeth RCiutac ŞtefanAinda não há avaliações
- Lateral Antrostomy For Max Sinus AugmentationDocumento9 páginasLateral Antrostomy For Max Sinus AugmentationsevattapillaiAinda não há avaliações
- PDF - BGB Contemporary Implant Dentistry PDFDocumento2 páginasPDF - BGB Contemporary Implant Dentistry PDFRadu FojicaAinda não há avaliações
- Facial Implants in Cosmetic SurgeryDocumento42 páginasFacial Implants in Cosmetic SurgeryMihada HashimAinda não há avaliações
- After Extraction InstructionDocumento4 páginasAfter Extraction Instructionmelly andrieAinda não há avaliações
- Consent in Orthodontics: Advice Sheet 4 British Orthodontic SocietyDocumento10 páginasConsent in Orthodontics: Advice Sheet 4 British Orthodontic SocietyfarisAinda não há avaliações
- CBCT Ch.7 DCNADocumento30 páginasCBCT Ch.7 DCNAgibsonAinda não há avaliações
- Rationale For Dental ImplantsDocumento18 páginasRationale For Dental ImplantsSamir Nayyar100% (1)
- Advancedtechniques Fordetectinglesions Inbone: Elisabetta CottiDocumento21 páginasAdvancedtechniques Fordetectinglesions Inbone: Elisabetta CottiAbdul Rahman AlmishhdanyAinda não há avaliações
- The Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsDocumento7 páginasThe Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsMárcia ChatelieAinda não há avaliações
- Immediate Implant Placement PDFDocumento11 páginasImmediate Implant Placement PDFFerdinan PasaribuAinda não há avaliações
- Maxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. HaugDocumento11 páginasMaxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. Hauglaura sanchez avilaAinda não há avaliações
- Straumann® Guided SurgeryDocumento58 páginasStraumann® Guided SurgerySupaluk Mod Chuencheep100% (1)
- Basic Surgical Principles With ITI ImplantsDocumento10 páginasBasic Surgical Principles With ITI ImplantsEliza DN100% (1)
- Craniofacial Bone Grafting Wolff's Law RevisitedDocumento13 páginasCraniofacial Bone Grafting Wolff's Law RevisitedR KAinda não há avaliações
- Armamentarium FOR Basic Oral Surgery: Deepthi P.R. Intern Dept. of Oral SurgeryDocumento140 páginasArmamentarium FOR Basic Oral Surgery: Deepthi P.R. Intern Dept. of Oral SurgeryGabriela Cocieru MotelicaAinda não há avaliações
- Computer-Assisted Craniomaxillofacial Surgery: Sean P. EdwardsDocumento18 páginasComputer-Assisted Craniomaxillofacial Surgery: Sean P. Edwardshasan nazzalAinda não há avaliações
- Implant Consent Form1Documento2 páginasImplant Consent Form1Jitender ReddyAinda não há avaliações
- Bicon Short Implant 3Documento6 páginasBicon Short Implant 3Bicon Implant InaAinda não há avaliações
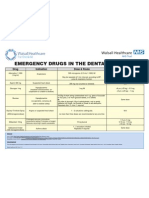
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocumento1 páginaEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefAinda não há avaliações
- First Page PDFDocumento1 páginaFirst Page PDFJordan BzAinda não há avaliações
- New Microsoft Office Word DocumentDocumento3 páginasNew Microsoft Office Word DocumentAtulsanapAinda não há avaliações
- Complications of Exodontics: Mary Cris P EstandarteDocumento49 páginasComplications of Exodontics: Mary Cris P EstandarteRealyn D. BerderaAinda não há avaliações
- Minor Surgical Procedures in Maxillofacial SurgeryDocumento65 páginasMinor Surgical Procedures in Maxillofacial SurgerydrzibranAinda não há avaliações
- Polyetheretherketone PEEK Dental Implants A Case FDocumento8 páginasPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- Oral Surgery FlapsDocumento13 páginasOral Surgery Flapshaneefmdf100% (1)
- Minimally Invasive Orthognathic SurgeryDocumento3 páginasMinimally Invasive Orthognathic SurgeryIJAR JOURNALAinda não há avaliações
- Manejo de Terceros Molares - Rafetto 2015Documento9 páginasManejo de Terceros Molares - Rafetto 2015Hugo HerreraAinda não há avaliações
- Boxer Fracture: An Unusual Presentation: KeywordsDocumento3 páginasBoxer Fracture: An Unusual Presentation: KeywordsRadita Dwihaning PutriAinda não há avaliações
- 208 342 1 SM PDFDocumento12 páginas208 342 1 SM PDFArisiaAinda não há avaliações
- NDT 67636 Comorbidity Between Obsessive Compulsive Disorder and Body D 082615Documento12 páginasNDT 67636 Comorbidity Between Obsessive Compulsive Disorder and Body D 082615Radita Dwihaning PutriAinda não há avaliações
- Update in Schizophrenia and Bipolar Disorder Focus On CariprazineDocumento6 páginasUpdate in Schizophrenia and Bipolar Disorder Focus On CariprazineRadita Dwihaning PutriAinda não há avaliações
- Jurnal BedahDocumento6 páginasJurnal BedahBrilliantineAinda não há avaliações
- Trends in Mental Health Care Among Children and AdolescentsDocumento10 páginasTrends in Mental Health Care Among Children and AdolescentsRadita Dwihaning PutriAinda não há avaliações
- Completion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessDocumento7 páginasCompletion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessRadita Dwihaning PutriAinda não há avaliações
- Macrolide Post FessDocumento7 páginasMacrolide Post FessDanti PutriAinda não há avaliações
- Clinical Study: Dog Bite Injuries: Primary and Secondary Emergency Department Presentations-A Retrospective Cohort StudyDocumento7 páginasClinical Study: Dog Bite Injuries: Primary and Secondary Emergency Department Presentations-A Retrospective Cohort StudyRadita Dwihaning PutriAinda não há avaliações
- Nasal Suction System For Endoscopic Sinus SurgeryDocumento3 páginasNasal Suction System For Endoscopic Sinus SurgeryRadita Dwihaning PutriAinda não há avaliações
- Ijohns 2015072715522054Documento6 páginasIjohns 2015072715522054Radita Dwihaning PutriAinda não há avaliações
- 1 s2.0 S0891584915003433 MainDocumento7 páginas1 s2.0 S0891584915003433 MainRadita Dwihaning PutriAinda não há avaliações
- Assessment of Quality of Life in Patients of Chronic RhinosinusitisDocumento4 páginasAssessment of Quality of Life in Patients of Chronic RhinosinusitisRadita Dwihaning PutriAinda não há avaliações
- Post Choclear ImplantationDocumento4 páginasPost Choclear ImplantationPhrycilia LimenAinda não há avaliações
- TCRM 0305 795Documento12 páginasTCRM 0305 795Radita Dwihaning PutriAinda não há avaliações
- OPTH 74555 Allergic Contact Dermatitis From Dorzolamide Eyedrops 040215Documento3 páginasOPTH 74555 Allergic Contact Dermatitis From Dorzolamide Eyedrops 040215Radita Dwihaning PutriAinda não há avaliações
- Bilateral Vocal Fold Immobility: A 13 Year Review of Etiologies, Management and The Utility of The Empey IndexDocumento7 páginasBilateral Vocal Fold Immobility: A 13 Year Review of Etiologies, Management and The Utility of The Empey IndexRadita Dwihaning PutriAinda não há avaliações
- IMCRJ 82679 Unilateral Corneal Leukoplakia Without Limbal Involvement 051815Documento4 páginasIMCRJ 82679 Unilateral Corneal Leukoplakia Without Limbal Involvement 051815Radita Dwihaning PutriAinda não há avaliações
- OPTH 45921 Diagnosis and Management of Neurotrophic Keratitis 031914Documento9 páginasOPTH 45921 Diagnosis and Management of Neurotrophic Keratitis 031914Radita Dwihaning PutriAinda não há avaliações
- Oral Chelators Deferasirox and Deferiprone For Transfusional Iron Overload in ThalasemiaDocumento7 páginasOral Chelators Deferasirox and Deferiprone For Transfusional Iron Overload in ThalasemiaRadita Dwihaning PutriAinda não há avaliações
- Comparative Efficacy of Desferrioxamine, Deferiprone and in ThalassemiaDocumento7 páginasComparative Efficacy of Desferrioxamine, Deferiprone and in ThalassemiaRadita Dwihaning PutriAinda não há avaliações
- Sequential Deferoxamine - Deferasirox in Treatment of MajorDocumento5 páginasSequential Deferoxamine - Deferasirox in Treatment of MajorRadita Dwihaning PutriAinda não há avaliações
- OPTH 69486 Clinical Utility of 3 Diquafosol Ophthalmic Solution in The 051515Documento8 páginasOPTH 69486 Clinical Utility of 3 Diquafosol Ophthalmic Solution in The 051515Radita Dwihaning PutriAinda não há avaliações
- Experience With Combination Therapy of Deferiprone and 2010Documento9 páginasExperience With Combination Therapy of Deferiprone and 2010Radita Dwihaning PutriAinda não há avaliações
- Efficacy of Combined Desferrioxamine and Deferiprone Versus Single 2009Documento4 páginasEfficacy of Combined Desferrioxamine and Deferiprone Versus Single 2009Radita Dwihaning PutriAinda não há avaliações
- Chelation Therapy With Oral Solution of 2013Documento4 páginasChelation Therapy With Oral Solution of 2013Radita Dwihaning PutriAinda não há avaliações
- Up 09Documento1 páginaUp 09Radita Dwihaning PutriAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar PustakaRadita Dwihaning PutriAinda não há avaliações
- Calcium and Oral Health: A Review: International Journal of Scientific Research September 2013Documento3 páginasCalcium and Oral Health: A Review: International Journal of Scientific Research September 2013Maqbul AlamAinda não há avaliações
- Studyplace Resto Comm DentSet 2Documento17 páginasStudyplace Resto Comm DentSet 2Zean TrainAinda não há avaliações
- Prevention of Dental DiseasesDocumento5 páginasPrevention of Dental DiseasesCentral Asian StudiesAinda não há avaliações
- 335375265-MCQ-in-Orthodontics - PDF Dentistry Bran PDFDocumento7 páginas335375265-MCQ-in-Orthodontics - PDF Dentistry Bran PDFHabeeb AL-AbsiAinda não há avaliações
- Management of An Infant Having Natal Teeth: Vishal Khandelwal, Ullal Anand Nayak, Prathibha Anand Nayak, Yash BafnaDocumento3 páginasManagement of An Infant Having Natal Teeth: Vishal Khandelwal, Ullal Anand Nayak, Prathibha Anand Nayak, Yash BafnabanyubiruAinda não há avaliações
- Nano DentistryDocumento6 páginasNano DentistryanugrasAinda não há avaliações
- (Reduced) 24th BaSS PREFINAL Program 2019Documento36 páginas(Reduced) 24th BaSS PREFINAL Program 2019Vera Radojkova NikolovskaAinda não há avaliações
- Clinical Dental Prosthetics by A Roy MacGregorDocumento364 páginasClinical Dental Prosthetics by A Roy MacGregorHanin Abukhiara75% (4)
- Developmental Disorders of Oral Cavity PDFDocumento121 páginasDevelopmental Disorders of Oral Cavity PDFMohammed Nabeel100% (1)
- Challacombe Scale ENGDocumento1 páginaChallacombe Scale ENGdianzalerti92400% (1)
- Begg1956 AJO DODocumento30 páginasBegg1956 AJO DOrohini venkateshAinda não há avaliações
- Lec 10 Technology of OperativeDocumento8 páginasLec 10 Technology of OperativeHassan TantawyAinda não há avaliações
- Abi VathyDocumento19 páginasAbi Vathynivitha naiduAinda não há avaliações
- Panchagavya Black Tooth Powder Is All You Need For All Your Dental ProblemsDocumento4 páginasPanchagavya Black Tooth Powder Is All You Need For All Your Dental ProblemsChandra Sekhar GajulaAinda não há avaliações
- Resin Composite 2Documento47 páginasResin Composite 2Kamal AhmedAinda não há avaliações
- NOTES SINUS LIFT PP PresentationDocumento3 páginasNOTES SINUS LIFT PP PresentationTuan NguyenAinda não há avaliações
- Basic Space MaintainersDocumento69 páginasBasic Space MaintainersOfier Siki0% (1)
- Topical Fluoride Nov 2019 IDA TIMESDocumento2 páginasTopical Fluoride Nov 2019 IDA TIMESDrMrsAyeshaKhushnoorAinda não há avaliações
- Hiral Abutment Selection Part 2Documento46 páginasHiral Abutment Selection Part 2khushbu samaniAinda não há avaliações
- SAP Bracket Placement PDFDocumento8 páginasSAP Bracket Placement PDFIsrael YumbayAinda não há avaliações
- Dentin Jurnal Kedokteran Gigi Vol V. No 1. April 2021: Amalia Mahpudhah, Isyana Erlita, Buyung MaglendaDocumento6 páginasDentin Jurnal Kedokteran Gigi Vol V. No 1. April 2021: Amalia Mahpudhah, Isyana Erlita, Buyung Maglendayuana dnsAinda não há avaliações
- Curriculum Vitae: DR - Marina FrancisDocumento3 páginasCurriculum Vitae: DR - Marina FrancisMarina JoelAinda não há avaliações
- MesializationDocumento7 páginasMesializationTesisTraduccionesRuzelAinda não há avaliações
- Pit and Fissure Sealants PDFDocumento180 páginasPit and Fissure Sealants PDFBBB HUYT100% (3)
- 04 Periodontal Morphology Components of The Alveolar BoneDocumento7 páginas04 Periodontal Morphology Components of The Alveolar BoneNaufal ThufailAinda não há avaliações
- Journal .Of Orthodontics and Oral Surgery: AmericanDocumento11 páginasJournal .Of Orthodontics and Oral Surgery: AmericanShirley AliagaAinda não há avaliações
- Management of Impacted Canine1Documento88 páginasManagement of Impacted Canine1Saumya Singh100% (1)
- Introduction To Dental Anatomy: Learning Objec TivesDocumento12 páginasIntroduction To Dental Anatomy: Learning Objec Tivesbalkiz mahamedAinda não há avaliações
- Ortho ReviewDocumento149 páginasOrtho ReviewCristina CisnerosAinda não há avaliações
- Root Canal Cover Up 1996 George MeinigDocumento238 páginasRoot Canal Cover Up 1996 George MeinigJayme100% (4)