Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Spe 2790 PaDocumento6 páginasSpe 2790 PaSharmilaa Suresh KannanAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- 648687Documento19 páginas648687Sharmilaa Suresh KannanAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- 1.1 Components of EnvironmentDocumento5 páginas1.1 Components of EnvironmentRathnavel Ponnuswami86% (36)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Natural Resources PDFDocumento37 páginasNatural Resources PDFAAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Atmospheric Environment: T.V. Ramachandra, ShwetmalaDocumento8 páginasAtmospheric Environment: T.V. Ramachandra, ShwetmalaSharmilaa Suresh KannanAinda não há avaliações
- Gravity Survey PDFDocumento9 páginasGravity Survey PDFDjayusmannugrahantoAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Emission Factors VehiclesDocumento89 páginasEmission Factors Vehiclessanthoshneo02@gmail.com0% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Disasters: Made By-Avyakth Challa (6F)Documento28 páginasDisasters: Made By-Avyakth Challa (6F)angeleshl5Ainda não há avaliações
- Indian Emission Regulation BookletDocumento61 páginasIndian Emission Regulation BookletSyed MajeedAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- 1.4 Energy FlowDocumento7 páginas1.4 Energy FlowRathnavel Ponnuswami100% (1)
- Chapter 5Documento51 páginasChapter 5dayasanuAinda não há avaliações
- Multi Disciplinary Nature of EnvironmentDocumento13 páginasMulti Disciplinary Nature of Environmentrajasantosh100% (1)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
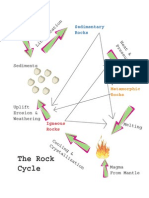
- Rock CycleDocumento1 páginaRock CycleDr.Jekyll363Ainda não há avaliações
- Density of MineralDocumento3 páginasDensity of MineralAjie RaharjoAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Ogunsola 1994Documento6 páginasOgunsola 1994Sharmilaa Suresh KannanAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Gulliver, Briggs - 2004 - Personal Exposure To Particulate Air Pollution in Transport Microenvironments - Atmospheric EnvironmentDocumento9 páginasGulliver, Briggs - 2004 - Personal Exposure To Particulate Air Pollution in Transport Microenvironments - Atmospheric EnvironmentSharmilaa Suresh KannanAinda não há avaliações
- Smit, Brown, Chan - 2008 - Do Air Pollution Emissions and Fuel Consumption Models For Roadways Include The Effects of Congestion in The RoadDocumento9 páginasSmit, Brown, Chan - 2008 - Do Air Pollution Emissions and Fuel Consumption Models For Roadways Include The Effects of Congestion in The RoadSharmilaa Suresh KannanAinda não há avaliações
- Geophysics Lecture NotesDocumento72 páginasGeophysics Lecture NotesNANKADAVUL007100% (1)
- Costabile, Allegrini - 2008 - A New Approach To Link Transport Emissions and Air Quality An Intelligent Transport System Based On The Contro PDFDocumento10 páginasCostabile, Allegrini - 2008 - A New Approach To Link Transport Emissions and Air Quality An Intelligent Transport System Based On The Contro PDFSharmilaa Suresh KannanAinda não há avaliações
- Environmental Science and Engineering Course OverviewDocumento2 páginasEnvironmental Science and Engineering Course OverviewSharmilaa Suresh KannanAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Bio FiltrationDocumento9 páginasBio FiltrationSharmilaa Suresh KannanAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- GE6351-Environmental Science and Engineering PDFDocumento7 páginasGE6351-Environmental Science and Engineering PDFSharmilaa Suresh KannanAinda não há avaliações
- A Methodology For Estimation of Vehicle Emissions in An Urban Environment An Example From Great ManchesterDocumento8 páginasA Methodology For Estimation of Vehicle Emissions in An Urban Environment An Example From Great ManchesterSharmilaa Suresh KannanAinda não há avaliações
- Textbook of Environment Studies For Undergraduate Courses - Erach Bharucha PDFDocumento260 páginasTextbook of Environment Studies For Undergraduate Courses - Erach Bharucha PDFPari Athouba100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- A Review of Traffic-Related Air Pollution Exposure Assessment Studies in The Developing WorldDocumento15 páginasA Review of Traffic-Related Air Pollution Exposure Assessment Studies in The Developing WorldSharmilaa Suresh KannanAinda não há avaliações
- EHEDocumento6 páginasEHESharmilaa Suresh KannanAinda não há avaliações
- Title of The Paper: Water Supply Engineering Subject Code: 11CBCI54Documento1 páginaTitle of The Paper: Water Supply Engineering Subject Code: 11CBCI54Sharmilaa Suresh KannanAinda não há avaliações
- Impact of Treated Grey Water On Physical and Chemical and Soil Characteristics"Documento83 páginasImpact of Treated Grey Water On Physical and Chemical and Soil Characteristics"Sharmilaa Suresh KannanAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Relationship To Continuum MechanicsDocumento5 páginasRelationship To Continuum MechanicsSharmilaa Suresh KannanAinda não há avaliações
- Transmission Line Basic PresentationDocumento141 páginasTransmission Line Basic PresentationSomiran Das100% (3)
- Puting Bato XXXDocumento9 páginasPuting Bato XXXMay Angelie QuindaoAinda não há avaliações
- Floor Coat Emulsion Platinum Series 1 PDFDocumento2 páginasFloor Coat Emulsion Platinum Series 1 PDFAalaya Housing Private LimitedAinda não há avaliações
- Haunted Wreck ScenarioDocumento1 páginaHaunted Wreck ScenarioPsygnosis ReddevilsAinda não há avaliações
- The Spirit's WisdomDocumento6 páginasThe Spirit's WisdomMike RigginsAinda não há avaliações
- Putting English To Work 1 - Unit 20Documento14 páginasPutting English To Work 1 - Unit 20komanjoeAinda não há avaliações
- L1Importance of Irrigation and DrainageDocumento18 páginasL1Importance of Irrigation and DrainagemimahmoudAinda não há avaliações
- Typical Schematic For Single Hot Water Heat PumpDocumento12 páginasTypical Schematic For Single Hot Water Heat PumpVin Bds100% (1)
- Conley - Climate Change Will Reshape Russia - Center For Strategic and International StudiesDocumento17 páginasConley - Climate Change Will Reshape Russia - Center For Strategic and International StudiesCarlos AyalaAinda não há avaliações
- 1 Cold WX Refresher PDFDocumento30 páginas1 Cold WX Refresher PDFallex_nathanielAinda não há avaliações
- Problem Set - MidtermDocumento3 páginasProblem Set - MidtermJohn Paul JacalanAinda não há avaliações
- Reading - Writing Booklet Term 2 Grade 3Documento29 páginasReading - Writing Booklet Term 2 Grade 3Mai Salem100% (1)
- Disaster Risk Reduction Exam PrepDocumento6 páginasDisaster Risk Reduction Exam PrepVerna M. Reyes100% (3)
- Top 10 Hurricane Preparedness Practices For Construction SitesDocumento7 páginasTop 10 Hurricane Preparedness Practices For Construction SitesMike KarlinsAinda não há avaliações
- Edible Iowa River Valley #17, Harvest 2010Documento36 páginasEdible Iowa River Valley #17, Harvest 2010k_frieseAinda não há avaliações
- Preparation of Genomic DNA From Mammalian TissuesDocumento3 páginasPreparation of Genomic DNA From Mammalian Tissuesraffaelec123Ainda não há avaliações
- Oddball Approach ChartsDocumento6 páginasOddball Approach ChartsGooreshAinda não há avaliações
- Stand Alone Photovoltaic SystemsDocumento438 páginasStand Alone Photovoltaic SystemsClearMind8450% (4)
- Malankara Plantations' 25kW Off-Grid Solar Power PlantDocumento6 páginasMalankara Plantations' 25kW Off-Grid Solar Power Plantguru jiAinda não há avaliações
- Ant Pad58 32 Data SheetDocumento2 páginasAnt Pad58 32 Data Sheetalfred calaunanAinda não há avaliações
- Test Bank For Introductory Statistics Exploring The World Through Data 0321891937Documento37 páginasTest Bank For Introductory Statistics Exploring The World Through Data 0321891937petaledrevealer155f100% (12)
- International Council For Research and Innovation in Building and Construction Working Commission W18 - Timber StructuresDocumento444 páginasInternational Council For Research and Innovation in Building and Construction Working Commission W18 - Timber Structuresaerodanger100% (1)
- Hot and Dry Climate of IndiaDocumento19 páginasHot and Dry Climate of Indiakhushi bansalAinda não há avaliações
- Heat Mass TransferDocumento5 páginasHeat Mass Transferlampshade17Ainda não há avaliações
- Summer TrainingDocumento33 páginasSummer TrainingManoj Shah100% (1)
- Time Series Analysis Components Trends Seasonal Cyclic RandomDocumento48 páginasTime Series Analysis Components Trends Seasonal Cyclic Randomcaamitthapa100% (1)
- Learn the 10 Heavenly Stems of BaZi with this color-coded guideDocumento9 páginasLearn the 10 Heavenly Stems of BaZi with this color-coded guideajakuk100% (1)
- Curriculum For General Knowledge 4 and 5Documento21 páginasCurriculum For General Knowledge 4 and 5jamaliah aliAinda não há avaliações
- Wind Energy Investigation in Northern Part of Kudat, MalaysiaDocumento9 páginasWind Energy Investigation in Northern Part of Kudat, MalaysiaAliashim Albani AllianAinda não há avaliações
- The Rights of Nature: A Legal Revolution That Could Save the WorldNo EverandThe Rights of Nature: A Legal Revolution That Could Save the WorldNota: 5 de 5 estrelas5/5 (1)
- Down to the Wire: Confronting Climate CollapseNo EverandDown to the Wire: Confronting Climate CollapseNota: 4.5 de 5 estrelas4.5/5 (8)
- Introduction to Ecology and Environmental Laws in IndiaNo EverandIntroduction to Ecology and Environmental Laws in IndiaAinda não há avaliações
- Principles of direct and superior responsibility in international humanitarian lawNo EverandPrinciples of direct and superior responsibility in international humanitarian lawAinda não há avaliações
- 3rd Grade Science: Life Sciences in Eco Systems | Textbook EditionNo Everand3rd Grade Science: Life Sciences in Eco Systems | Textbook EditionAinda não há avaliações
- Art of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionNo EverandArt of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionNota: 3 de 5 estrelas3/5 (1)