Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Dental Referral FormDocumento1 páginaDental Referral FormJade M. LolongAinda não há avaliações
- S2 2013 323973 BibliographyDocumento6 páginasS2 2013 323973 BibliographyJade M. LolongAinda não há avaliações
- Association of Environmental Tobacco Smoke and Snacking Habits With The Risk of Early Childhood Caries Among 3-Year-Old Japanese ChildrenDocumento6 páginasAssociation of Environmental Tobacco Smoke and Snacking Habits With The Risk of Early Childhood Caries Among 3-Year-Old Japanese ChildrenJade M. LolongAinda não há avaliações
- G PulpDocumento9 páginasG PulpwindhaAinda não há avaliações
- Ghazal Factors Associated With Early Childhood Caries Incidence Among High Caries-Risk ChildrenDocumento9 páginasGhazal Factors Associated With Early Childhood Caries Incidence Among High Caries-Risk ChildrenJade M. LolongAinda não há avaliações
- Observed Child and Parent Tooth Brushing Behaviors and Child Oral HealthDocumento9 páginasObserved Child and Parent Tooth Brushing Behaviors and Child Oral HealthJade M. LolongAinda não há avaliações
- Managing Carious LesionsDocumento1 páginaManaging Carious LesionsJade M. LolongAinda não há avaliações
- Clinical Evaluation of Root Canal Obturation Methods in Primary TeethDocumento9 páginasClinical Evaluation of Root Canal Obturation Methods in Primary TeethJade M. LolongAinda não há avaliações
- To Pack or Not To Pack: The Current Status of Periodontal DressingsDocumento14 páginasTo Pack or Not To Pack: The Current Status of Periodontal DressingsJade M. LolongAinda não há avaliações
- Subcutaneous Emphysema During Third Molar Surgery: A Case ReportDocumento4 páginasSubcutaneous Emphysema During Third Molar Surgery: A Case ReportEdric MichaelAinda não há avaliações
- Palatal Perforation Secondary To Tuberculosis A Case ReportDocumento3 páginasPalatal Perforation Secondary To Tuberculosis A Case ReportJade M. LolongAinda não há avaliações
- Preparation of Adhesive Inlays and Onlays.Documento5 páginasPreparation of Adhesive Inlays and Onlays.Jade M. LolongAinda não há avaliações
- Evaluation of Fractured Condylar Head Along The Sagittal Plane Report of Three CasesDocumento4 páginasEvaluation of Fractured Condylar Head Along The Sagittal Plane Report of Three CasesJade M. LolongAinda não há avaliações
- Policy On Oral HabitsDocumento2 páginasPolicy On Oral HabitsJade M. LolongAinda não há avaliações
- Occlusal Plane Location in Edentulous Patients A ReviewDocumento7 páginasOcclusal Plane Location in Edentulous Patients A ReviewJade M. Lolong50% (2)
- Rehabilitation of Atrophic Maxilla A Review of 101 Zygomatic ImplantsDocumento8 páginasRehabilitation of Atrophic Maxilla A Review of 101 Zygomatic ImplantsJade M. LolongAinda não há avaliações
- Osteomyelitis of The Mandible in A Patient With Osteopetrosis Case Report and Review of The LiteratureDocumento6 páginasOsteomyelitis of The Mandible in A Patient With Osteopetrosis Case Report and Review of The LiteratureJade M. LolongAinda não há avaliações
- Spring-Bite: A New Device For Jaw Motion Rehabilitation. A Case ReportDocumento4 páginasSpring-Bite: A New Device For Jaw Motion Rehabilitation. A Case ReportJade M. LolongAinda não há avaliações
- Comparacao Entre TecnicasDocumento14 páginasComparacao Entre TecnicasjoserodrrAinda não há avaliações
- Case Report of Difficult Dental Prosthesis Insertion Due To Severe Gag ReflexDocumento7 páginasCase Report of Difficult Dental Prosthesis Insertion Due To Severe Gag ReflexJade M. LolongAinda não há avaliações
- Location and Presence of Permanent Teeth in A Complete Bilateral Cleft Lip and Palate PopulationDocumento6 páginasLocation and Presence of Permanent Teeth in A Complete Bilateral Cleft Lip and Palate PopulationJade M. LolongAinda não há avaliações
- Occlusal Plane Location in Edentulous Patients A ReviewDocumento7 páginasOcclusal Plane Location in Edentulous Patients A ReviewJade M. Lolong50% (2)
- Ceph HandoutDocumento18 páginasCeph Handoutwaheguru13he13Ainda não há avaliações
- Preliminary Impressions in Microstomia Patients An InnovativeDocumento4 páginasPreliminary Impressions in Microstomia Patients An InnovativeJade M. LolongAinda não há avaliações
- Candida-Associated Denture StomatitisDocumento5 páginasCandida-Associated Denture StomatitisJade M. LolongAinda não há avaliações
- Tabel IotnDocumento3 páginasTabel IotnPuspita PutriAinda não há avaliações
- Eur J Orthod 2002 Hunt 53 9Documento8 páginasEur J Orthod 2002 Hunt 53 9Jade M. LolongAinda não há avaliações
- Ceph TracingDocumento1 páginaCeph TracingJade M. LolongAinda não há avaliações
- Luxation InjuriesDocumento4 páginasLuxation InjuriesJade M. LolongAinda não há avaliações
- Alternatives Thiomersal Preservatives VaccinesDocumento15 páginasAlternatives Thiomersal Preservatives VaccinesHerdiwan NovindraAinda não há avaliações
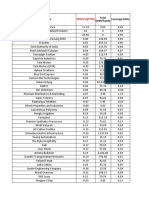
- Data of ReportsDocumento539 páginasData of ReportsArjun LakhaniAinda não há avaliações
- WHO Pharmaceuticals Newsletter No 3 2023 1693146010Documento18 páginasWHO Pharmaceuticals Newsletter No 3 2023 1693146010vivek rakhaAinda não há avaliações
- Theoretical YieldDocumento8 páginasTheoretical YieldIzzatul HidayahAinda não há avaliações
- Argumentative EssaysDocumento7 páginasArgumentative EssaysSarah Tasnia100% (1)
- Hypertensive Urgency: University of Perpetual Help System DALTA - Las PiñasDocumento8 páginasHypertensive Urgency: University of Perpetual Help System DALTA - Las PiñasJustin HericoAinda não há avaliações
- Celgene January 2019 Investor-PresentationDocumento26 páginasCelgene January 2019 Investor-PresentationmedtechyAinda não há avaliações
- Department of Health and Human Services: Food and Drug AdministrationDocumento50 páginasDepartment of Health and Human Services: Food and Drug AdministrationlosangelesAinda não há avaliações
- Omidian 12 Book ChapterDocumento31 páginasOmidian 12 Book ChapterAlina DAinda não há avaliações
- The World of Science and Innovation 14 16.01.2021Documento1.289 páginasThe World of Science and Innovation 14 16.01.2021Костя ДолинськийAinda não há avaliações
- Diphereline S.R 3.75mg EngDocumento3 páginasDiphereline S.R 3.75mg EngBotond BarthaAinda não há avaliações
- SakajajaDocumento34 páginasSakajajavini nurbaitiAinda não há avaliações
- BASF PS Pharma Produktkatalog UPDATE WEBDocumento44 páginasBASF PS Pharma Produktkatalog UPDATE WEBAhmad SaputraAinda não há avaliações
- HIV/AIDS Symptoms and SignsDocumento3 páginasHIV/AIDS Symptoms and SignsAmin MofrehAinda não há avaliações
- Pharma 3Documento7 páginasPharma 3Uday kumarAinda não há avaliações
- 2004 Chem 2OB3 Lab Manual - Experiment 4. Reactions of Carboxylic AcidsDocumento4 páginas2004 Chem 2OB3 Lab Manual - Experiment 4. Reactions of Carboxylic AcidsNstm3Ainda não há avaliações
- GlaxoSmithkline Merger (ODA)Documento20 páginasGlaxoSmithkline Merger (ODA)Shaukat HassaniAinda não há avaliações
- Chapter ReviewDocumento32 páginasChapter ReviewThanh TrúcAinda não há avaliações
- Vipul Doshi - Compliance Road MapDocumento49 páginasVipul Doshi - Compliance Road Mapkumar_chemical100% (1)
- Prilling and GranulationDocumento56 páginasPrilling and GranulationMuhammad SaddamAinda não há avaliações
- Dendrimers: A Review: January 2010Documento6 páginasDendrimers: A Review: January 2010Jesús Antonio Cruz NavarroAinda não há avaliações
- T1K UpdateDocumento24 páginasT1K UpdateolivenanaAinda não há avaliações
- Managing Otitis ExternaDocumento34 páginasManaging Otitis ExternaramaAinda não há avaliações
- 2001 AnnualDocumento78 páginas2001 Annualrizaldi rahmatullahAinda não há avaliações
- Formulation and Evaluation of Tablet of Nicardipine HCL As A Solid Self-Emulsifying Drug Delivery SystemDocumento6 páginasFormulation and Evaluation of Tablet of Nicardipine HCL As A Solid Self-Emulsifying Drug Delivery SystemWJPSR JournalAinda não há avaliações
- 1 Polypharmacy Facts and FiguresDocumento10 páginas1 Polypharmacy Facts and Figuresghostanime2002Ainda não há avaliações
- Briviact 75 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC)Documento12 páginasBriviact 75 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC)Rutvik Patel - F&DAinda não há avaliações
- Pharmacodynamics of AntibioticsDocumento28 páginasPharmacodynamics of AntibioticsHazimMahmoudDarwishAinda não há avaliações
- Example of Product Leaflet's AssignmentDocumento6 páginasExample of Product Leaflet's AssignmentFarah Adilah AdeniAinda não há avaliações
- IV To PO Antibiotic Step Down GuidelinesDocumento1 páginaIV To PO Antibiotic Step Down GuidelinesGayle GreyAinda não há avaliações