Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Evaluation of The Microbotox Technique An.12Documento10 páginasEvaluation of The Microbotox Technique An.12Blessing KelechiAinda não há avaliações
- Quantec Vs Emami Discussion PostDocumento1 páginaQuantec Vs Emami Discussion Postapi-374655242Ainda não há avaliações
- Pneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahaDocumento50 páginasPneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahappgpcsAinda não há avaliações
- Vaccination CentersDocumento4 páginasVaccination CentersdmonlinelkAinda não há avaliações
- Risks of Self-Medication Practices: October 2010Documento28 páginasRisks of Self-Medication Practices: October 2010Matiyas ZewdeAinda não há avaliações
- Bahasa Inggris (NARKOBA)Documento7 páginasBahasa Inggris (NARKOBA)jimtumangkeAinda não há avaliações
- Quanti-Cult Plus ENG Dos PasesDocumento4 páginasQuanti-Cult Plus ENG Dos Pasessagor sagorAinda não há avaliações
- Nursing Care Plan Funds 2Documento7 páginasNursing Care Plan Funds 2Yash RamawatAinda não há avaliações
- Is Rashes A Symptom of Pregnancy - Google SearchDocumento1 páginaIs Rashes A Symptom of Pregnancy - Google SearchCovenant UbahAinda não há avaliações
- TORCH Infection in Pregnant Women Ver September 2017 PDFDocumento9 páginasTORCH Infection in Pregnant Women Ver September 2017 PDFRevina AmaliaAinda não há avaliações
- Hearing-Impairment Case StudyDocumento10 páginasHearing-Impairment Case StudyIrish Eunice Felix100% (1)
- Acute and Chronic SinusitisDocumento39 páginasAcute and Chronic SinusitissuciAinda não há avaliações
- Reinforcement in Checking Vital SignsDocumento7 páginasReinforcement in Checking Vital SignsFarah FildzahAinda não há avaliações
- IFU NormaCont3+ EDocumento1 páginaIFU NormaCont3+ Ethuy dinhAinda não há avaliações
- Overview of Gastrointestinal Tract PerforationDocumento37 páginasOverview of Gastrointestinal Tract PerforationArbujeloAinda não há avaliações
- Epidemiological ApproachDocumento47 páginasEpidemiological ApproachPrem Deep100% (1)
- Bedside Emergency Cardiac Ultrasound in ChildrenDocumento11 páginasBedside Emergency Cardiac Ultrasound in ChildrenNikhil KumarAinda não há avaliações
- Conversation ExerciseDocumento4 páginasConversation ExerciseMbarr DiantoeAinda não há avaliações
- Grade 6 - SSES - Science - Q2 - Wk2 - GLAKDocumento16 páginasGrade 6 - SSES - Science - Q2 - Wk2 - GLAKMelanie TrinidadAinda não há avaliações
- UHS Syllabus With TOS (3rd Syllabus With TOS Year MBBS) Syllabus With TOS)Documento26 páginasUHS Syllabus With TOS (3rd Syllabus With TOS Year MBBS) Syllabus With TOS)Ali AhmadAinda não há avaliações
- Terapi 2Documento7 páginasTerapi 2emma sitahAinda não há avaliações
- ECMO, Adults BJA 2011Documento5 páginasECMO, Adults BJA 2011RAGHAVENDRA VAGYANNAVARAinda não há avaliações
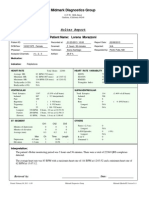
- Full Report Holter Lorena M 1-23-13Documento36 páginasFull Report Holter Lorena M 1-23-13traja_vlrAinda não há avaliações
- Emotional Body Pain Chart: How It WorksDocumento3 páginasEmotional Body Pain Chart: How It Worksdaniel50% (2)
- Tugas MetodeDocumento8 páginasTugas MetodeEllya Latifah IlyasAinda não há avaliações
- Reviewer Fundamentals of NursingDocumento22 páginasReviewer Fundamentals of NursingDarren Flores100% (1)
- CDC: Obesity Approaching Tobacco As Top Preventable Cause of DeathDocumento2 páginasCDC: Obesity Approaching Tobacco As Top Preventable Cause of DeathSanti PadmasariAinda não há avaliações
- EPISIOTOMYDocumento17 páginasEPISIOTOMYKaye Arriane TenorioAinda não há avaliações
- CH 25 Mycoplasma and UreaplasmaDocumento14 páginasCH 25 Mycoplasma and UreaplasmashericeAinda não há avaliações