Você também pode gostar
- Molecular, Genetic, and Nutritional Aspects of Major and Trace MineralsNo EverandMolecular, Genetic, and Nutritional Aspects of Major and Trace MineralsAinda não há avaliações
- The Emerging Role of The Liver in Iron Metabolism: Clinical ReviewsDocumento6 páginasThe Emerging Role of The Liver in Iron Metabolism: Clinical ReviewsYuriko BoringAinda não há avaliações
- Iron Tutorial Introduction To IronDocumento11 páginasIron Tutorial Introduction To Ironmonday125Ainda não há avaliações
- Hepcidin - Central Regulator of Iron MetabolismDocumento10 páginasHepcidin - Central Regulator of Iron MetabolismQistina SudarnotoAinda não há avaliações
- Iron AbsorptionDocumento3 páginasIron AbsorptionmaiiiAinda não há avaliações
- ThesisDocumento26 páginasThesisMaryam AbdelkarimAinda não há avaliações
- Hematology 2009 Zhang 207 14Documento8 páginasHematology 2009 Zhang 207 14Yuvens RichardoAinda não há avaliações
- Hepatic Iron Metabolism - Anderson-Frazer 2005Documento13 páginasHepatic Iron Metabolism - Anderson-Frazer 2005kocagerahmetAinda não há avaliações
- Pathophysiology of Iron HomeostasisDocumento10 páginasPathophysiology of Iron HomeostasisJoséDantasAinda não há avaliações
- Untitled DocumentDocumento5 páginasUntitled DocumentAnn MariaAinda não há avaliações
- Metabolism FeDocumento17 páginasMetabolism Feeduardo sosaAinda não há avaliações
- Mechanisms Controlling Cellular - Nature Ncoa4 Ekim23Documento23 páginasMechanisms Controlling Cellular - Nature Ncoa4 Ekim23kocagerahmetAinda não há avaliações
- 03 Iron Transport Proteins Gateways of Cellular and SystemicDocumento9 páginas03 Iron Transport Proteins Gateways of Cellular and SystemicMatheus SouzaAinda não há avaliações
- Iron Physiology of IronDocumento7 páginasIron Physiology of IronAnna PodsiadłoAinda não há avaliações
- The Role of Hepatic Transferrin Receptor 2 in The Regulation of Iron Homeostasis in The BodyDocumento8 páginasThe Role of Hepatic Transferrin Receptor 2 in The Regulation of Iron Homeostasis in The BodyherunoviatAinda não há avaliações
- Lo 7Documento5 páginasLo 7Sitha Medha ParamithaAinda não há avaliações
- FerritinDocumento15 páginasFerritinericmeitei100% (1)
- IronDocumento22 páginasIronJoiceLanaAinda não há avaliações
- Iron HomeostasisDocumento30 páginasIron HomeostasisTony NgAinda não há avaliações
- Mechanisms of Iron Loading and Toxicity: Gregory J. AndersonDocumento4 páginasMechanisms of Iron Loading and Toxicity: Gregory J. Andersonikhsan07Ainda não há avaliações
- Metabolisme IronDocumento15 páginasMetabolisme IronERNI FORWATYAinda não há avaliações
- Metabolites 12 00609 v2Documento11 páginasMetabolites 12 00609 v2Ionela MariaAinda não há avaliações
- Subject ChemistryDocumento12 páginasSubject ChemistrykottooranjohnbAinda não há avaliações
- Trace ElementsDocumento10 páginasTrace ElementsJim Lloyd MulitAinda não há avaliações
- Intestinal Absorption of Iron in HFE-1 Hemochromatosis Local or Systemic ProcessDocumento8 páginasIntestinal Absorption of Iron in HFE-1 Hemochromatosis Local or Systemic ProcessMădălina CiobotariuAinda não há avaliações
- InorganicDocumento34 páginasInorganicManWol JangAinda não há avaliações
- An Assignment On Basic BiochemistryDocumento12 páginasAn Assignment On Basic BiochemistrySamira RahmanAinda não há avaliações
- Balance de HierroDocumento13 páginasBalance de HierroWalter Huacani HuamaniAinda não há avaliações
- Iron Kinetics and Laboratory AssessmentDocumento4 páginasIron Kinetics and Laboratory AssessmentJohnree A. EvangelistaAinda não há avaliações
- Iron Metabolism and DiseaseDocumento50 páginasIron Metabolism and DiseaseHeet MewadaAinda não há avaliações
- CB Chapter 13 IronDocumento16 páginasCB Chapter 13 IronPaulina PaskeviciuteAinda não há avaliações
- Regulation of Iron MetabolismDocumento21 páginasRegulation of Iron MetabolismElita Maritan SAinda não há avaliações
- Lecture 3 - Iron Homeostasis, AnemiaDocumento30 páginasLecture 3 - Iron Homeostasis, AnemiaJoanna BrumaruAinda não há avaliações
- Bahan ReferatDocumento6 páginasBahan ReferatGoldenbird 120494Ainda não há avaliações
- Diagnosis and Management of Iron Deficiency Anemia in The 21st CenturyDocumento8 páginasDiagnosis and Management of Iron Deficiency Anemia in The 21st CenturyireneAinda não há avaliações
- Hematinic PreparationsDocumento19 páginasHematinic PreparationsAbdur RaquibAinda não há avaliações
- 04 - Iron Homeostasis in Host DefenceDocumento11 páginas04 - Iron Homeostasis in Host DefenceMatheus SouzaAinda não há avaliações
- Hepcidin Regulation of Iron TransportDocumento5 páginasHepcidin Regulation of Iron TransportQistina SudarnotoAinda não há avaliações
- Iron MetabolismDocumento43 páginasIron Metabolismrabiatahir421Ainda não há avaliações
- Asian Paci Fic Journal of Tropical Medicine: Iron Dysregulation in Beta-ThalassemiaDocumento9 páginasAsian Paci Fic Journal of Tropical Medicine: Iron Dysregulation in Beta-ThalassemiafitriahendricoAinda não há avaliações
- NeuroergonomicDocumento19 páginasNeuroergonomicrifqi_udinAinda não há avaliações
- RON Etabolism: Compartment % Iron ContentDocumento4 páginasRON Etabolism: Compartment % Iron ContentReiner John S. HermoginoAinda não há avaliações
- Group G Assignment On Microminerals (Iron and Iodine)Documento20 páginasGroup G Assignment On Microminerals (Iron and Iodine)melesse bisemaAinda não há avaliações
- Globular Proteins: Dr. Sujin Bao, SJSMDocumento27 páginasGlobular Proteins: Dr. Sujin Bao, SJSMethanAinda não há avaliações
- Human Iron Metabolism - WikipediaDocumento37 páginasHuman Iron Metabolism - WikipediaMaysaa AlashkarAinda não há avaliações
- HHS Public Access: Ironing Out FerroportinDocumento24 páginasHHS Public Access: Ironing Out FerroportinMădălina CiobotariuAinda não há avaliações
- A Saga of Hepcidin Anti-Microbial Effectiveness As Iron Acquisitor and Anemia Initiator in Mycobacterium Tuberculosis InfectionDocumento7 páginasA Saga of Hepcidin Anti-Microbial Effectiveness As Iron Acquisitor and Anemia Initiator in Mycobacterium Tuberculosis InfectionidhaAinda não há avaliações
- Biochemical PharmacologyDocumento9 páginasBiochemical PharmacologyArifAinda não há avaliações
- 1 s2.0 S0171933522000334 MainDocumento12 páginas1 s2.0 S0171933522000334 Main4-005-กิตติ์การต์ วีราพิสิษฐ์Ainda não há avaliações
- Experiment 6 (Irone and Transferrin)Documento19 páginasExperiment 6 (Irone and Transferrin)photo copyhemnAinda não há avaliações
- Iron BalanceDocumento7 páginasIron BalancegigibesiAinda não há avaliações
- Hepcidin, The Iron WatcherDocumento6 páginasHepcidin, The Iron WatcherQistina SudarnotoAinda não há avaliações
- Functions of Iron-Overview: e Donor and AcceptorDocumento41 páginasFunctions of Iron-Overview: e Donor and AcceptorLuiza RadulescuAinda não há avaliações
- Lec 1 InorganicDocumento33 páginasLec 1 Inorganiciam2117Ainda não há avaliações
- 3758 1 5371 1 10 20121126Documento8 páginas3758 1 5371 1 10 20121126raniAinda não há avaliações
- Minerals Iron by Dr. Faisal Hassan Shah (06.04.2020)Documento141 páginasMinerals Iron by Dr. Faisal Hassan Shah (06.04.2020)Laraib SohailAinda não há avaliações
- Hum. Mol. Genet.-2009-Ramsay-3673-83Documento11 páginasHum. Mol. Genet.-2009-Ramsay-3673-83Aniki PuspitaAinda não há avaliações
- Elemetal Iron Not RecommendedDocumento11 páginasElemetal Iron Not RecommendedSegun TalabiAinda não há avaliações
- Iron Kinetics and Laboratory AssessmentDocumento24 páginasIron Kinetics and Laboratory AssessmentWissam AlwazaniAinda não há avaliações
- Minerals: Trace ElementsDocumento182 páginasMinerals: Trace ElementsSaad KhanAinda não há avaliações
- Mitosis Final Demo PresentationDocumento59 páginasMitosis Final Demo PresentationJames PalomariaAinda não há avaliações
- BCH MCQs1Documento304 páginasBCH MCQs1moxdegr8100% (1)
- Metabolism of XenobioticsDocumento4 páginasMetabolism of XenobioticsChingHuaAinda não há avaliações
- 5.the Genetic CodeDocumento8 páginas5.the Genetic CodeCharm BatiancilaAinda não há avaliações
- Grade 8 Science TQ 4th PrelimDocumento2 páginasGrade 8 Science TQ 4th PrelimAngel DPAinda não há avaliações
- Unit 3 - Cell Energy Guided NotesDocumento3 páginasUnit 3 - Cell Energy Guided NotesKaylee Lopez Student - KnightdaleHSAinda não há avaliações
- ATP Photosynthesis and Cell Respiration Web QuestDocumento3 páginasATP Photosynthesis and Cell Respiration Web QuestJakie UbinaAinda não há avaliações
- Nucleolus A Central Hub For Nuclear FunctionsDocumento13 páginasNucleolus A Central Hub For Nuclear FunctionsJuan Andres Fernández MAinda não há avaliações
- Post Translational Modification PPT SlideshareDocumento13 páginasPost Translational Modification PPT SlideshareWaqas KhalidAinda não há avaliações
- Chromosomal Structure and Chromosomal MutationsDocumento28 páginasChromosomal Structure and Chromosomal MutationsKavisa GhoshAinda não há avaliações
- AQA Biology A-Level - Cell Cycle and Mitosis QPDocumento22 páginasAQA Biology A-Level - Cell Cycle and Mitosis QPMuffin CAinda não há avaliações
- J Jacc 2007 02 059v1Documento17 páginasJ Jacc 2007 02 059v1maestro1234567890Ainda não há avaliações
- Chapter 6: Cell Division: 6.3: MEIOSISDocumento29 páginasChapter 6: Cell Division: 6.3: MEIOSISMohammed RidzuwanAinda não há avaliações
- Paper Transcription & Translation: Proteins: MlelrlvqgsllkkvleairDocumento5 páginasPaper Transcription & Translation: Proteins: MlelrlvqgsllkkvleairXimena QuenguanAinda não há avaliações
- Computational Prediction and Characterization of miRNA From Coconut Leaf TranscriptomeDocumento6 páginasComputational Prediction and Characterization of miRNA From Coconut Leaf TranscriptomeShailendra RajanAinda não há avaliações
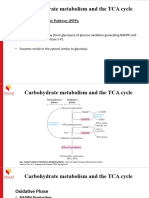
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Documento17 páginasCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelAinda não há avaliações
- 2007 Pan, Discovery of Selective Irreversible Inhibitors For Bruton's Tyrosine KinaseDocumento4 páginas2007 Pan, Discovery of Selective Irreversible Inhibitors For Bruton's Tyrosine KinaseYesid EstupiñanAinda não há avaliações
- Chapter 3. Invitro Growth of Oocyte and Oocyte Maturation Đã Chuyển ĐổiDocumento49 páginasChapter 3. Invitro Growth of Oocyte and Oocyte Maturation Đã Chuyển ĐổiGia HoàngAinda não há avaliações
- What I Know: Quarter 2 - Module 1 Energy TransformationDocumento8 páginasWhat I Know: Quarter 2 - Module 1 Energy TransformationLyka Mae BenitoAinda não há avaliações
- Cytokines: C:/CD DATA/all Collection notes/IMMUNOLOGY/cytokines - Doc - 1Documento6 páginasCytokines: C:/CD DATA/all Collection notes/IMMUNOLOGY/cytokines - Doc - 1vishal patelAinda não há avaliações
- Mitosis and Meiosis: Bio Lab-131 Session-Fall 2021 Section-001Documento27 páginasMitosis and Meiosis: Bio Lab-131 Session-Fall 2021 Section-001Satya NadellaAinda não há avaliações
- Central DogmaDocumento50 páginasCentral DogmaIvilyn ManguladAinda não há avaliações
- Csir Net NotesDocumento63 páginasCsir Net Notesssjusvinder75% (4)
- Quarter 3-DNA SCIENCE 10Documento29 páginasQuarter 3-DNA SCIENCE 10Rubeliza LawengAinda não há avaliações
- Cell Bio Exam 2 Lecure QuizzesDocumento42 páginasCell Bio Exam 2 Lecure QuizzesHafiza Dia Islam100% (4)
- Perbedaan MCF 7 Dan t47dDocumento9 páginasPerbedaan MCF 7 Dan t47dmuflihAinda não há avaliações
- Practicals - Term II PDF 1 CLASS 12 BIODocumento13 páginasPracticals - Term II PDF 1 CLASS 12 BIOAmaanAinda não há avaliações
- Central Dogma Worksheet 2Documento2 páginasCentral Dogma Worksheet 2josh VillanuevaAinda não há avaliações
- CC 11 3611Documento16 páginasCC 11 3611Sergeat18BAinda não há avaliações
- Mindmap DnaDocumento7 páginasMindmap Dnafresh wooAinda não há avaliações
- It's Elemental: The Hidden Chemistry in EverythingNo EverandIt's Elemental: The Hidden Chemistry in EverythingNota: 4 de 5 estrelas4/5 (10)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactNo EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactNota: 5 de 5 estrelas5/5 (5)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincNo EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincNota: 3.5 de 5 estrelas3.5/5 (137)
- AP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeNo EverandAP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeNota: 5 de 5 estrelas5/5 (1)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeNo EverandChemistry for Breakfast: The Amazing Science of Everyday LifeNota: 4.5 de 5 estrelas4.5/5 (14)
- Taste: Surprising Stories and Science About Why Food Tastes GoodNo EverandTaste: Surprising Stories and Science About Why Food Tastes GoodNota: 3 de 5 estrelas3/5 (20)
- Guidelines for Defining Process Safety Competency RequirementsNo EverandGuidelines for Defining Process Safety Competency RequirementsNota: 3 de 5 estrelas3/5 (1)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeNo EverandChemistry for Breakfast: The Amazing Science of Everyday LifeNota: 4.5 de 5 estrelas4.5/5 (90)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeNo EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeNota: 5 de 5 estrelas5/5 (4)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeNo EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeNota: 4 de 5 estrelas4/5 (1)
- AP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeNo EverandAP Chemistry Flashcards, Fourth Edition: Up-to-Date Review and PracticeAinda não há avaliações
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideNo EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideAinda não há avaliações
- The Periodic Table: A Very Short IntroductionNo EverandThe Periodic Table: A Very Short IntroductionNota: 4.5 de 5 estrelas4.5/5 (3)
- Tribology: Friction and Wear of Engineering MaterialsNo EverandTribology: Friction and Wear of Engineering MaterialsNota: 5 de 5 estrelas5/5 (1)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsNo EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsNota: 4 de 5 estrelas4/5 (146)
- Guidelines for Integrating Process Safety into Engineering ProjectsNo EverandGuidelines for Integrating Process Safety into Engineering ProjectsAinda não há avaliações
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsNo EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsAinda não há avaliações
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactNo EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactNota: 5 de 5 estrelas5/5 (1)
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolNo EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolAinda não há avaliações
- Ingredients: A Visual Exploration of 75 Additives & 25 Food ProductsNo EverandIngredients: A Visual Exploration of 75 Additives & 25 Food ProductsNota: 4 de 5 estrelas4/5 (1)