Você também pode gostar
- Endocrine PhysiologyDocumento98 páginasEndocrine PhysiologyMohan GuptaAinda não há avaliações
- Hormonal Agents PharmacologyDocumento64 páginasHormonal Agents Pharmacologynica velanoAinda não há avaliações
- Metabolic & Endocrine DiseasesDocumento280 páginasMetabolic & Endocrine DiseasesHussenAinda não há avaliações
- 4 Pituitary HormonesDocumento18 páginas4 Pituitary HormonesRana AbdullahAinda não há avaliações
- Hypothalamus and Pituitary Gland FunctionsDocumento48 páginasHypothalamus and Pituitary Gland FunctionsMohsin AbbasAinda não há avaliações
- Hormones 080623Documento83 páginasHormones 080623Rao Asad MubeenAinda não há avaliações
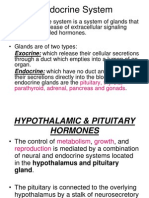
- Endocrine System: Endocrine: Which Have No Duct and ReleaseDocumento36 páginasEndocrine System: Endocrine: Which Have No Duct and Releasedr_saleh77Ainda não há avaliações
- Regulasi Endokrin 22 IntensifDocumento25 páginasRegulasi Endokrin 22 IntensifWignes WarenAinda não há avaliações
- Endocrine SystemDocumento69 páginasEndocrine SystemDivya JaiswalAinda não há avaliações
- Hypothalamus & Pituitary GlandDocumento39 páginasHypothalamus & Pituitary GlandVishal DodejaAinda não há avaliações
- Reproductive SystemDocumento114 páginasReproductive SystemIsha NagleAinda não há avaliações
- 2 HZ Hypothalamic and Pituitary Hormones HZDocumento20 páginas2 HZ Hypothalamic and Pituitary Hormones HZAmirabbas SaffariAinda não há avaliações
- Hormonal BiochemistryDocumento82 páginasHormonal BiochemistryRuthAinda não há avaliações
- 11 - Chem Coordination and Integration PDFDocumento37 páginas11 - Chem Coordination and Integration PDFAAinda não há avaliações
- LECTURE 1 Endocrine Diseases Lecture 1 January 10-020Documento68 páginasLECTURE 1 Endocrine Diseases Lecture 1 January 10-020aleen qawareetAinda não há avaliações
- Endocrine DrugsDocumento172 páginasEndocrine DrugsAlvim Tiel FactorAinda não há avaliações
- BSC Anterior Pituitary HormonesDocumento27 páginasBSC Anterior Pituitary HormonesThalapathy PrakashAinda não há avaliações
- Pharmacology: EndocrineDocumento210 páginasPharmacology: EndocrineSharifa Darayan100% (1)
- 22. Chemical Co Ordination and Integration_434dea34 f494 4704 a8c9 6876397e324eDocumento53 páginas22. Chemical Co Ordination and Integration_434dea34 f494 4704 a8c9 6876397e324epcgurukotari9Ainda não há avaliações
- Hormones of the Endocrine System: An OverviewDocumento51 páginasHormones of the Endocrine System: An OverviewGutu Garemewu BiruAinda não há avaliações
- Hypothalamic and Pituitary Drugs (Autosaved)Documento41 páginasHypothalamic and Pituitary Drugs (Autosaved)mug ashAinda não há avaliações
- Anterior Pituitary (Autosaved)Documento33 páginasAnterior Pituitary (Autosaved)BABLU GAMINGAinda não há avaliações
- Maher Khdour, PHD: Associate Prof. Faculty of Pharmacy Al-Quds UniversityDocumento52 páginasMaher Khdour, PHD: Associate Prof. Faculty of Pharmacy Al-Quds Universityتمارا عكاري.Ainda não há avaliações
- 3rd BSC Endocrinology NotesDocumento25 páginas3rd BSC Endocrinology NotesPratyashaAinda não há avaliações
- Endocrine SystemDocumento96 páginasEndocrine SystemSandhya Kakkar100% (2)
- Biochemistry of Hormones (Part 1)Documento31 páginasBiochemistry of Hormones (Part 1)arun231187Ainda não há avaliações
- Pituitary and ThyroidDocumento54 páginasPituitary and ThyroidSaif AliAinda não há avaliações
- Endocrinology Apllied ScienceDocumento44 páginasEndocrinology Apllied ScienceAdam PrabowoAinda não há avaliações
- 22 Chemical Co-OrdinationDocumento47 páginas22 Chemical Co-OrdinationRachna JaiswalAinda não há avaliações
- Module 22 HormonesDocumento23 páginasModule 22 HormonesCrystal ManguneAinda não há avaliações
- HORMONESDocumento65 páginasHORMONESsoumya palavalasaAinda não há avaliações
- Hormonal Regulation of MetabolismDocumento80 páginasHormonal Regulation of MetabolismVivek ChaudharyAinda não há avaliações
- Endocrine System - MorphophysiologyDocumento88 páginasEndocrine System - MorphophysiologyKarina Bustillo100% (1)
- Endocrinology Endocrinology: H. KibichoDocumento370 páginasEndocrinology Endocrinology: H. KibichoMursal RashidAinda não há avaliações
- ENDOCRINE SYSTEM DISORDERS PROPER best (1)Documento370 páginasENDOCRINE SYSTEM DISORDERS PROPER best (1)ronaronixstheboyAinda não há avaliações
- The Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewDocumento27 páginasThe Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewEdelrose LapitanAinda não há avaliações
- Chapter 10Documento3 páginasChapter 10Zoe DorothyAinda não há avaliações
- Group 9 (Module 22)Documento24 páginasGroup 9 (Module 22)maba.zuniga.sjcAinda não há avaliações
- Endocrine System GuideDocumento37 páginasEndocrine System GuideKochaMsangiAinda não há avaliações
- T3 Ans PDFDocumento62 páginasT3 Ans PDFMiles HuiAinda não há avaliações
- The Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1Documento12 páginasThe Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1lourd nabAinda não há avaliações
- BIOLS372. (21) Endocrinology SummaryDocumento15 páginasBIOLS372. (21) Endocrinology SummaryNawaf Al.RiffaiAinda não há avaliações
- Ila College of Health: Endocrine PhysiologyDocumento40 páginasIla College of Health: Endocrine PhysiologyDaniel DendaAinda não há avaliações
- Unit IXDocumento10 páginasUnit IXPreeti ChouhanAinda não há avaliações
- The Endocrine SystemDocumento7 páginasThe Endocrine SystemcystanarisaAinda não há avaliações
- Chemical Signals in Animals: Egg Larva Pupa AdultDocumento29 páginasChemical Signals in Animals: Egg Larva Pupa AdultMENWER ALJOHANIAinda não há avaliações
- EndocrinologyDocumento74 páginasEndocrinologysyedahaleemajunaidsAinda não há avaliações
- Endocrine ReviewDocumento9 páginasEndocrine ReviewSpencer ThomasAinda não há avaliações
- General Principles of Metabolism Regulation. HormonesDocumento90 páginasGeneral Principles of Metabolism Regulation. HormonesМохіт Кумар ЯмпатіAinda não há avaliações
- 6 Hormones Secreted by The AdenohypophysisDocumento5 páginas6 Hormones Secreted by The Adenohypophysischristine_8995Ainda não há avaliações
- BMSN2202 Life Science II Year 2, 5 Year Curriculum Tutorial 3 PhysiologyDocumento61 páginasBMSN2202 Life Science II Year 2, 5 Year Curriculum Tutorial 3 PhysiologyMiles HuiAinda não há avaliações
- Endocrine SystemDocumento31 páginasEndocrine SystemPreeti ChouhanAinda não há avaliações
- Pituitary Gland: Prepared by Yousaf KhanDocumento19 páginasPituitary Gland: Prepared by Yousaf KhanSalman KhanAinda não há avaliações
- The Endocrine System: An Overview of Key Hormones and Their FunctionsDocumento38 páginasThe Endocrine System: An Overview of Key Hormones and Their FunctionsAngelika ButaslacAinda não há avaliações
- Hormones:: Signaling MoleculesDocumento20 páginasHormones:: Signaling MoleculesSangeeta DwivediAinda não há avaliações
- A&PII Test 1Documento14 páginasA&PII Test 1Alyssa BattcockAinda não há avaliações
- Endocrine PhysiologyDocumento76 páginasEndocrine Physiologykidusabeje7Ainda não há avaliações
- Endocrine Physiology For Pharmacy Students-2023Documento118 páginasEndocrine Physiology For Pharmacy Students-2023Alemnew YohannesAinda não há avaliações
- GIFTED: Genetic Information For Treating Eating DisordersNo EverandGIFTED: Genetic Information For Treating Eating DisordersAinda não há avaliações
- European Vol-32 No-6 2011Documento15 páginasEuropean Vol-32 No-6 2011mahaberani_zAinda não há avaliações
- Parkinsonism (巴金森氏症) and other movement disordersDocumento29 páginasParkinsonism (巴金森氏症) and other movement disordersShing Ming TangAinda não há avaliações
- Mezoterapija PDFDocumento11 páginasMezoterapija PDFDavid DijakAinda não há avaliações
- Bone Grafting: Classification by OriginDocumento4 páginasBone Grafting: Classification by OriginHerlangga Fadhillah AkbarAinda não há avaliações
- Jessica Hughes AP Biology LabDocumento8 páginasJessica Hughes AP Biology LabJessica HughesAinda não há avaliações
- Colorectal Cancer A ReviewDocumento11 páginasColorectal Cancer A ReviewMarcelitaTaliaDuwiriAinda não há avaliações
- Preanalytical Variability Associated With The Procurement and Study of Small Biopsies - 091022dwDocumento19 páginasPreanalytical Variability Associated With The Procurement and Study of Small Biopsies - 091022dwkamulegeya RogersAinda não há avaliações
- Pathophysiology Respiratory SystemDocumento63 páginasPathophysiology Respiratory SystemAli Basha QudahAinda não há avaliações
- Syndrome in PsychiatryDocumento12 páginasSyndrome in Psychiatryrahul KumarAinda não há avaliações
- Anatomy & PhysiologyDocumento12 páginasAnatomy & PhysiologyTyrAinda não há avaliações
- Msds Heksana - 2 PDFDocumento6 páginasMsds Heksana - 2 PDFrilmaAinda não há avaliações
- Basic Risk MeasurementDocumento18 páginasBasic Risk Measurementgoku krishnaAinda não há avaliações
- MictobsDocumento7 páginasMictobsAnuja AnushaAinda não há avaliações
- Sistem Otot Dan Kerangka UnggasDocumento20 páginasSistem Otot Dan Kerangka UnggasWahyu Solhan MaghfurAinda não há avaliações
- Control of Breathing and Acute Respiratory Failure: PearlsDocumento6 páginasControl of Breathing and Acute Respiratory Failure: PearlsbuburuzaoAinda não há avaliações
- @medicinejournal American Journal of Perinatology September 2017Documento128 páginas@medicinejournal American Journal of Perinatology September 2017angsukriAinda não há avaliações
- Biomedical Research To Improve The Lives of People With Down SyndromeDocumento13 páginasBiomedical Research To Improve The Lives of People With Down SyndromeGlobalDownSyndromeAinda não há avaliações
- Seminar On Cancer: Submitted To Submitted byDocumento13 páginasSeminar On Cancer: Submitted To Submitted byUdaya SreeAinda não há avaliações
- Biochemical and Molecular Characterization of The Venom From The Cuban Scorpion Rhopalurus JunceusDocumento10 páginasBiochemical and Molecular Characterization of The Venom From The Cuban Scorpion Rhopalurus JunceusCapitulina AmbrioletaAinda não há avaliações
- Dissocial Personality DisorderDocumento52 páginasDissocial Personality DisorderSam InvincibleAinda não há avaliações
- NBME CompDocumento7 páginasNBME CompWinter Ohio100% (4)
- Medical Terminology of Blood, Lymphatic and Immune SystemsDocumento5 páginasMedical Terminology of Blood, Lymphatic and Immune Systemssotman58Ainda não há avaliações
- Antigen Processing and Presentation 09Documento34 páginasAntigen Processing and Presentation 09Khairul Ikhwan100% (2)
- PharmacoDocumento20 páginasPharmacoBrian OkariAinda não há avaliações
- Type IV Hypersensitivity - WikipediaDocumento3 páginasType IV Hypersensitivity - WikipediaLokesh BakshiAinda não há avaliações
- Incredible Italian Brand-New Ocean LinerDocumento1 páginaIncredible Italian Brand-New Ocean LinerTrisha Park100% (1)
- Tools of BioinformaticsDocumento29 páginasTools of BioinformaticsM HaroonAinda não há avaliações
- MIT White Paper On ConvergenceDocumento40 páginasMIT White Paper On ConvergenceChuin-Shan David ChenAinda não há avaliações
- Inheritance of Sex and Sex-Linked or Influenced Traits - StudentDocumento21 páginasInheritance of Sex and Sex-Linked or Influenced Traits - StudentNoob Gamer0% (1)
- Filipino BiologistsDocumento2 páginasFilipino BiologistsMaine MaruzzoAinda não há avaliações