Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Peer Support: Community Mental Health Good Practice GuideDocumento24 páginasPeer Support: Community Mental Health Good Practice GuideMark Lobo100% (1)
- What Are Peer Recovery Support Services?Documento17 páginasWhat Are Peer Recovery Support Services?The Stacie Mathewson FoundationAinda não há avaliações
- Best of The Best Spartanburg Winners 2022Documento1 páginaBest of The Best Spartanburg Winners 2022UploadedbyHaroldGaterAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Peer Support Training ManualDocumento126 páginasPeer Support Training ManualTrent DavisAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Funeral Home LawsuitDocumento14 páginasFuneral Home LawsuitUploadedbyHaroldGater100% (1)
- Justin L. Smith StatementDocumento4 páginasJustin L. Smith StatementUploadedbyHaroldGaterAinda não há avaliações
- Speech by U.S. Judge Carlton ReevesDocumento16 páginasSpeech by U.S. Judge Carlton ReevesUploadedbyHaroldGater100% (1)
- Tenn. State Rep. Torrey Harris ComplaintDocumento1 páginaTenn. State Rep. Torrey Harris ComplaintUploadedbyHaroldGaterAinda não há avaliações
- 2021-22 Headcount Enrollment by College Level Gender and Race EthnicityDocumento1 página2021-22 Headcount Enrollment by College Level Gender and Race EthnicityUploadedbyHaroldGaterAinda não há avaliações
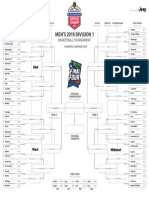
- 2019 NCAA Tournament BracketDocumento1 página2019 NCAA Tournament BracketUSA TODAY Network100% (1)
- Mueller ReportDocumento448 páginasMueller ReportStefan Becket95% (165)
- Letter To Gov. Tate Reeves On House Bill 382 FinalDocumento2 páginasLetter To Gov. Tate Reeves On House Bill 382 FinalUploadedbyHaroldGaterAinda não há avaliações
- 2019 Mississippi Sales Tax HolidayDocumento4 páginas2019 Mississippi Sales Tax HolidayUploadedbyHaroldGaterAinda não há avaliações
- Jay-Z, Yo Gotti Lawsuit Against Top Mississippi Prison OfficialDocumento11 páginasJay-Z, Yo Gotti Lawsuit Against Top Mississippi Prison OfficialUploadedbyHaroldGater100% (2)
- If You Don't See Your State Representative or Senator On This List, Please Contact Them and Encourage Them Not To Attend The ConferenceDocumento2 páginasIf You Don't See Your State Representative or Senator On This List, Please Contact Them and Encourage Them Not To Attend The ConferenceUploadedbyHaroldGaterAinda não há avaliações
- 2018 Measuring Up To The ModelDocumento118 páginas2018 Measuring Up To The ModelUploadedbyHaroldGaterAinda não há avaliações
- 2019 NCAA Women's Basketball Tournament BracketDocumento1 página2019 NCAA Women's Basketball Tournament BracketUSA TODAY NetworkAinda não há avaliações
- Beth Poff Zoo LetterDocumento3 páginasBeth Poff Zoo LetterUploadedbyHaroldGaterAinda não há avaliações
- David Watkins IndictmentDocumento2 páginasDavid Watkins IndictmentUploadedbyHaroldGaterAinda não há avaliações
- 03-26-18 Remember Mississippi Chris McDaniel Complaint #MssenDocumento31 páginas03-26-18 Remember Mississippi Chris McDaniel Complaint #MssenRuss LatinoAinda não há avaliações
- Proposed Mississippi Sports Betting RulesDocumento21 páginasProposed Mississippi Sports Betting RulesUploadedbyHaroldGaterAinda não há avaliações
- Notice of ClaimDocumento3 páginasNotice of ClaimUploadedbyHaroldGater0% (1)
- Malone FileDocumento6 páginasMalone Filethe kingfishAinda não há avaliações
- JPS Takeover LawsuitDocumento41 páginasJPS Takeover Lawsuitthe kingfishAinda não há avaliações
- Clyde Kennard ComicDocumento15 páginasClyde Kennard ComicUploadedbyHaroldGaterAinda não há avaliações
- Houston Nutt's Lawsuit Against Ole MissDocumento21 páginasHouston Nutt's Lawsuit Against Ole MissJay Hart100% (2)
- Rankin IndictmentsDocumento6 páginasRankin Indictmentsthe kingfishAinda não há avaliações
- Madison County Sheriff Response To LawsuitDocumento47 páginasMadison County Sheriff Response To LawsuitUploadedbyHaroldGaterAinda não há avaliações
- Brown v. Madison County ACLU of MS ComplaintDocumento86 páginasBrown v. Madison County ACLU of MS ComplaintUploadedbyHaroldGaterAinda não há avaliações
- Farrar NOA Response RedactedDocumento29 páginasFarrar NOA Response RedactedJay HartAinda não há avaliações
- R Kelly LawsuitDocumento18 páginasR Kelly LawsuitUploadedbyHaroldGaterAinda não há avaliações
- Rebel Rags ComplaintDocumento9 páginasRebel Rags ComplaintUploadedbyHaroldGater100% (1)
- Final Desk Review Report - SupervisionDocumento20 páginasFinal Desk Review Report - SupervisionBishal SahaAinda não há avaliações
- NLF - Ending An American Tragedy 2009Documento8 páginasNLF - Ending An American Tragedy 2009ttcoffeyAinda não há avaliações
- The Pathway To Employment Framework FINAL 2Documento23 páginasThe Pathway To Employment Framework FINAL 2laili nikAinda não há avaliações
- Key Considerations in Delivering Trauma-Informed Professional Learning For EducatorsDocumento8 páginasKey Considerations in Delivering Trauma-Informed Professional Learning For EducatorsViolacea LowAinda não há avaliações
- Covid 19Documento23 páginasCovid 19Ika nur masitohAinda não há avaliações
- Psychosis and Schizophrenia in Adult - NICE GuidelineDocumento39 páginasPsychosis and Schizophrenia in Adult - NICE Guidelineyuliana160793Ainda não há avaliações
- 2019 PSRANM Conference Program FinalDocumento24 páginas2019 PSRANM Conference Program FinalKimmie JordanAinda não há avaliações
- Original Research Ikwara Et Al, 2024Documento31 páginasOriginal Research Ikwara Et Al, 2024charlesokello.the1stAinda não há avaliações
- The RECOVER Project - From The Ground Up - How To Build Your Own Peer-To-peer Recovery CentreDocumento109 páginasThe RECOVER Project - From The Ground Up - How To Build Your Own Peer-To-peer Recovery CentrePaul CAinda não há avaliações
- Fall 05Documento6 páginasFall 05Nick LuchettiAinda não há avaliações
- Asca Ethical StandardsDocumento12 páginasAsca Ethical Standardsapi-641678125Ainda não há avaliações
- LongBeach Psych PostdocDocumento18 páginasLongBeach Psych PostdocdrerwinsAinda não há avaliações
- Peer Support: For Student Mental HealthDocumento22 páginasPeer Support: For Student Mental HealthJohanna BibartAinda não há avaliações
- RCE Wellbeing Hub: Everything You Need To Know AboutDocumento20 páginasRCE Wellbeing Hub: Everything You Need To Know AboutNikos LolisAinda não há avaliações
- Reminder ARCHES Recovery College Jan-Feb-Mar 2023 ProgrammeDocumento5 páginasReminder ARCHES Recovery College Jan-Feb-Mar 2023 ProgrammeGateway ProjectAinda não há avaliações
- Un Women Brief Prevention Violence Against Women and Girls and Covid 19 enDocumento8 páginasUn Women Brief Prevention Violence Against Women and Girls and Covid 19 ensofiabloemAinda não há avaliações
- WASP 2019 Final ProgrammeDocumento18 páginasWASP 2019 Final ProgrammeAlexandra PopaAinda não há avaliações
- 2 17+-+Zimbabwe+CATS+-+long+form+-+1 13 18Documento10 páginas2 17+-+Zimbabwe+CATS+-+long+form+-+1 13 18Rumbidzai MurwisiAinda não há avaliações
- Clare Foster CVDocumento2 páginasClare Foster CVfostressAinda não há avaliações
- Shenandoah County Resource Updated 01 2022Documento2 páginasShenandoah County Resource Updated 01 2022api-659222337Ainda não há avaliações
- Peer SupportDocumento1 páginaPeer SupportsarahAinda não há avaliações
- FinalintegrativereviewDocumento17 páginasFinalintegrativereviewapi-346349076Ainda não há avaliações
- Peer Support Specialist ResumeDocumento7 páginasPeer Support Specialist Resumeafllufama100% (1)
- Enhancing Peer Support - Liane Angel KalacasDocumento18 páginasEnhancing Peer Support - Liane Angel KalacasEdgardo T. GaliciaAinda não há avaliações
- Post-Diagnostic Support For People Living With DementiaDocumento13 páginasPost-Diagnostic Support For People Living With DementiadionisioAinda não há avaliações
- Domestic ViolenceDocumento10 páginasDomestic ViolenceShinsha SaleemAinda não há avaliações
- Awareness About Remedial MeasuresDocumento2 páginasAwareness About Remedial MeasuresAsma AzamAinda não há avaliações