Você também pode gostar
- Assignment AnswersDocumento6 páginasAssignment Answersbebo4gpaAinda não há avaliações
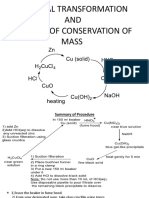
- Chemical Transformation AND The Law of Conservation of MassDocumento2 páginasChemical Transformation AND The Law of Conservation of Massbebo4gpaAinda não há avaliações
- Effect of Gamma-Irradiation On Thermal Decomposition of Tris (1,2-Diaminoethane) Cobalt (II) SulphateDocumento6 páginasEffect of Gamma-Irradiation On Thermal Decomposition of Tris (1,2-Diaminoethane) Cobalt (II) Sulphatebebo4gpaAinda não há avaliações
- Multistep 2Documento4 páginasMultistep 2bebo4gpaAinda não há avaliações
- Studies On Synthesis and Characterization of Some Novel Aromatic Copolyesters Based On S-TriazineDocumento9 páginasStudies On Synthesis and Characterization of Some Novel Aromatic Copolyesters Based On S-Triazinebebo4gpaAinda não há avaliações
- Chalcones, Pyrazolines and Aminopyrimidines As Antibacterial AgentsDocumento5 páginasChalcones, Pyrazolines and Aminopyrimidines As Antibacterial Agentsbebo4gpaAinda não há avaliações
- Reactions of TrichlorotriazineDocumento16 páginasReactions of Trichlorotriazinebebo4gpaAinda não há avaliações
- Lab 6: Base Extraction of Benzoic Acid From Acetanilide Followed by Recrystallization and MP DeterminationDocumento9 páginasLab 6: Base Extraction of Benzoic Acid From Acetanilide Followed by Recrystallization and MP Determinationbebo4gpaAinda não há avaliações
- Polymer Nanocomposites For Aerospace Applications: CharacterizationDocumento7 páginasPolymer Nanocomposites For Aerospace Applications: Characterizationbebo4gpaAinda não há avaliações
- Type of Transformation Reagents Special NotesDocumento1 páginaType of Transformation Reagents Special Notesbebo4gpaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- SSP 465 12l 3 Cylinder Tdi Engine With Common Rail Fuel Injection SystemDocumento56 páginasSSP 465 12l 3 Cylinder Tdi Engine With Common Rail Fuel Injection SystemJose Ramón Orenes ClementeAinda não há avaliações
- Public Conveyances: Environments in Public and Enclosed Places"Documento1 páginaPublic Conveyances: Environments in Public and Enclosed Places"Jesse Joe LagonAinda não há avaliações
- Menu Siklus RSDocumento3 páginasMenu Siklus RSChika VionitaAinda não há avaliações
- Sol. Mock Test CBSE BiologyDocumento3 páginasSol. Mock Test CBSE BiologysbarathiAinda não há avaliações
- Wilo Water PumpDocumento16 páginasWilo Water PumpThit SarAinda não há avaliações
- Boeco BM-800 - User ManualDocumento21 páginasBoeco BM-800 - User ManualJuan Carlos CrespoAinda não há avaliações
- Kingdom of AnimaliaDocumento6 páginasKingdom of AnimaliaBen ZerepAinda não há avaliações
- EM2U60CLP 115-127 V 60 HZ 1Documento4 páginasEM2U60CLP 115-127 V 60 HZ 1armagedrumAinda não há avaliações
- Schematic Diagram For Pharmaceutical Water System 1652323261Documento1 páginaSchematic Diagram For Pharmaceutical Water System 1652323261Ankit SinghAinda não há avaliações
- Faraz Chem ProjectDocumento13 páginasFaraz Chem ProjectFaraz AhmedAinda não há avaliações
- MCQ Homework: PeriodonticsDocumento4 páginasMCQ Homework: Periodonticsفراس الموسويAinda não há avaliações
- L Addison Diehl-IT Training ModelDocumento1 páginaL Addison Diehl-IT Training ModelL_Addison_DiehlAinda não há avaliações
- Muscle and Fitness Hers Features Elite Lifestyle Chef Carlo FilipponeDocumento4 páginasMuscle and Fitness Hers Features Elite Lifestyle Chef Carlo FilipponeCarlo FilipponeAinda não há avaliações
- Online Games and Academic AchievementDocumento25 páginasOnline Games and Academic AchievementJasmine GamoraAinda não há avaliações
- BR Interlock Pallet Racking System 2009 enDocumento8 páginasBR Interlock Pallet Racking System 2009 enMalik Rehan SyedAinda não há avaliações
- PPC Production PlantDocumento106 páginasPPC Production PlantAljay Neeson Imperial100% (1)
- Total Elbow Arthroplasty and RehabilitationDocumento5 páginasTotal Elbow Arthroplasty and RehabilitationMarina EAinda não há avaliações
- TCJ Series: TCJ Series - Standard and Low Profile - J-LeadDocumento14 páginasTCJ Series: TCJ Series - Standard and Low Profile - J-LeadgpremkiranAinda não há avaliações
- Hmo Details November 2022 1Documento6 páginasHmo Details November 2022 1Saad BelloAinda não há avaliações
- 99 AutomaticDocumento6 páginas99 AutomaticDustin BrownAinda não há avaliações
- Powerful Communication Tools For Successful Acupuncture PracticeDocumento4 páginasPowerful Communication Tools For Successful Acupuncture Practicebinglei chenAinda não há avaliações
- BCA2006 BCA GuideDocumento507 páginasBCA2006 BCA GuidePatrick LiaoAinda não há avaliações
- Thorley Amended Complaint (Signed)Documento13 páginasThorley Amended Complaint (Signed)Heather ClemenceauAinda não há avaliações
- Constantino V MendezDocumento3 páginasConstantino V MendezNīc CādīgālAinda não há avaliações
- EscheatmentDocumento58 páginasEscheatmentlaarigao100% (2)
- Cyber Safety PP Presentation For Class 11Documento16 páginasCyber Safety PP Presentation For Class 11WAZ CHANNEL100% (1)
- User Manual: 3603807 CONTACT US - 09501447202,8070690001Documento1 páginaUser Manual: 3603807 CONTACT US - 09501447202,8070690001Arokiaraj RajAinda não há avaliações
- OKRA Standards For UKDocumento8 páginasOKRA Standards For UKabc111007100% (2)
- Operational Safety and Health Procedures, Practices and RegulationsDocumento20 páginasOperational Safety and Health Procedures, Practices and RegulationsDionisa ErnacioAinda não há avaliações
- L A R G e - S C A L e M e T H A M P H e T A M I N e M A N U F A C T U R eDocumento21 páginasL A R G e - S C A L e M e T H A M P H e T A M I N e M A N U F A C T U R eDaria Schka100% (1)