Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Fundamentals of NursingDocumento29 páginasFundamentals of Nursingblazegomez92% (26)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Job DescriptionDocumento10 páginasJob Descriptionpioneer92Ainda não há avaliações
- Soap CardiologyDocumento155 páginasSoap CardiologyTambunta Tarigan100% (5)
- 10 1016@j Ihj 2017 04 007Documento5 páginas10 1016@j Ihj 2017 04 007Tambunta TariganAinda não há avaliações
- DEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011Documento110 páginasDEPKES RI NEW Pedoman Nasional Penanggulangan TBC 2011familyman8091% (11)
- Gui Mares 2016Documento7 páginasGui Mares 2016Tambunta TariganAinda não há avaliações
- Prognostic Value of Red Blood Cell Distribution Width in Heart Failure Patients - A Meta-AnalysisDocumento5 páginasPrognostic Value of Red Blood Cell Distribution Width in Heart Failure Patients - A Meta-AnalysisTambunta TariganAinda não há avaliações
- Arbel2014 PDFDocumento4 páginasArbel2014 PDFTambunta TariganAinda não há avaliações
- Critical Appraisal Worksheet 3Documento3 páginasCritical Appraisal Worksheet 3Tambunta TariganAinda não há avaliações
- Log Book 2Documento21 páginasLog Book 2Tambunta TariganAinda não há avaliações
- FN 2011 IdsaDocumento38 páginasFN 2011 IdsaNuttawath UngwichanpunyaAinda não há avaliações
- Febrile Neutropenia Final 7-29Documento74 páginasFebrile Neutropenia Final 7-29Tambunta TariganAinda não há avaliações
- Ann Oncol 2010 de Naurois v252 6Documento5 páginasAnn Oncol 2010 de Naurois v252 6Tambunta TariganAinda não há avaliações
- Singh 2015Documento12 páginasSingh 2015Tambunta TariganAinda não há avaliações
- Smith 2016Documento9 páginasSmith 2016Tambunta TariganAinda não há avaliações
- Physiology Laboratory Evaluating Metabolic Syndrome in A MedicalDocumento5 páginasPhysiology Laboratory Evaluating Metabolic Syndrome in A MedicalTambunta TariganAinda não há avaliações
- BJMP 0908 NamasoodiDocumento4 páginasBJMP 0908 NamasoodiTambunta TariganAinda não há avaliações
- Mini Nutritional Assessment: ScreeningDocumento1 páginaMini Nutritional Assessment: ScreeningjinkuocsulbAinda não há avaliações
- 97managementstable AnginaDocumento20 páginas97managementstable AnginaTambunta TariganAinda não há avaliações
- Hodgkin Lymphoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Documento73 páginasHodgkin Lymphoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Tambunta TariganAinda não há avaliações
- Operating Room ProcedureDocumento6 páginasOperating Room ProcedureleviAinda não há avaliações
- Office: The of The SecretaryDocumento13 páginasOffice: The of The SecretaryJoseph RepotenteAinda não há avaliações
- CEO Analysis George Halvorson by Ryland HamletDocumento8 páginasCEO Analysis George Halvorson by Ryland HamletRyland HamletAinda não há avaliações
- NepahealthDocumento12 páginasNepahealthDixit PhuyalAinda não há avaliações
- APH Case StudyDocumento4 páginasAPH Case StudyandengAinda não há avaliações
- SB4 CheckpointDocumento2 páginasSB4 Checkpointทำไป เพื่ออะไรAinda não há avaliações
- CA Minor Consent Laws - Mental Health Services PDFDocumento5 páginasCA Minor Consent Laws - Mental Health Services PDFvictor assessingAinda não há avaliações
- Hospice Care PaperDocumento12 páginasHospice Care Paperapi-247160803100% (2)
- E-R Diagram Examples Questions PrintDocumento9 páginasE-R Diagram Examples Questions PrintGetachew ShambelAinda não há avaliações
- SEASAC Softball Girls Programme 2013Documento24 páginasSEASAC Softball Girls Programme 2013falconsnistAinda não há avaliações
- SSS Handbook PDFDocumento45 páginasSSS Handbook PDFsarahAinda não há avaliações
- ACUTE ABDOMEN Systemic SonographicDocumento6 páginasACUTE ABDOMEN Systemic SonographiciwanAinda não há avaliações
- Marcus Soos Accident April 19Documento3 páginasMarcus Soos Accident April 19api-310805543Ainda não há avaliações
- Platelet and Plasma Transfusion Policy. in Blood Transfusion Guideline PDFDocumento13 páginasPlatelet and Plasma Transfusion Policy. in Blood Transfusion Guideline PDFbencleeseAinda não há avaliações
- Readers Digest April 2015Documento146 páginasReaders Digest April 2015herbertjohn24100% (1)
- Effectiveness of Back Massage On Sleep Among Patients With Major Orthopedic Surgery in Selected Hospital, Nagercoil, Tamil NaDocumento9 páginasEffectiveness of Back Massage On Sleep Among Patients With Major Orthopedic Surgery in Selected Hospital, Nagercoil, Tamil NaInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- NursingDocumento3 páginasNursingTayyeba SyeddainAinda não há avaliações
- Koreksi Hiperkalemia - Julia K - EnGDocumento26 páginasKoreksi Hiperkalemia - Julia K - EnGJulia KasabAinda não há avaliações
- PruebaDocumento2 páginasPruebaHenry Guatemal CadenaAinda não há avaliações
- Tugas Bahasa Inggris 2 Per 1Documento4 páginasTugas Bahasa Inggris 2 Per 1Rori RevizaAinda não há avaliações
- Nurse Career Pathway ProjectDocumento3 páginasNurse Career Pathway ProjectcharlesAinda não há avaliações
- Children's Services Job DescriptionDocumento11 páginasChildren's Services Job DescriptionMuhammad Dian Luthfy LubisAinda não há avaliações
- B Bartholins Abscess - Word CatheterDocumento2 páginasB Bartholins Abscess - Word CatheterMuhammadUsriYusranAinda não há avaliações
- BBA Final Year ProjectDocumento80 páginasBBA Final Year ProjectSai Printers100% (3)
- Apply Ade Adrain SitompulDocumento6 páginasApply Ade Adrain Sitompulade adrain sitompulAinda não há avaliações
- AFLAC Cancer L3 BrochureDocumento8 páginasAFLAC Cancer L3 Brochuresunil singhAinda não há avaliações
- Leadership Behaviors of Frontline Staff NursesDocumento9 páginasLeadership Behaviors of Frontline Staff NursessatmayaniAinda não há avaliações
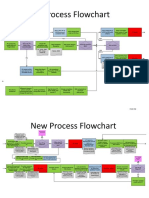
- New Process Flowchart CPOEDocumento4 páginasNew Process Flowchart CPOELiza GeorgeAinda não há avaliações