Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Vegemite KeyDocumento2 páginasVegemite KeykatybabyyyAinda não há avaliações
- Wall E Movie Questions PDFDocumento4 páginasWall E Movie Questions PDFkatybabyyyAinda não há avaliações
- Wall E Movie Questions PDFDocumento4 páginasWall E Movie Questions PDFkatybabyyyAinda não há avaliações
- Christmas Crossword PDFDocumento2 páginasChristmas Crossword PDFHana MusialovaAinda não há avaliações
- Brisbane Woman's Death Linked To Salmonella Outbreak On Melbourne Cup DayDocumento2 páginasBrisbane Woman's Death Linked To Salmonella Outbreak On Melbourne Cup DaykatybabyyyAinda não há avaliações
- School Subjects Esl Vocabulary Wordsearch Puzzle WorksheetDocumento2 páginasSchool Subjects Esl Vocabulary Wordsearch Puzzle WorksheetkatybabyyyAinda não há avaliações
- Information For ApplicantsDocumento15 páginasInformation For ApplicantskatybabyyyAinda não há avaliações
- TB Skin TestDocumento2 páginasTB Skin TestkatybabyyyAinda não há avaliações
- ABC of Management of Hypovolaemic Shock: Major TraumaDocumento5 páginasABC of Management of Hypovolaemic Shock: Major TraumakatybabyyyAinda não há avaliações
- 81 150 1 SM PDFDocumento2 páginas81 150 1 SM PDFkatybabyyyAinda não há avaliações
- BeadsDocumento43 páginasBeadskatybabyyyAinda não há avaliações
- Imovie Tip Sheet PDFDocumento1 páginaImovie Tip Sheet PDFkatybabyyyAinda não há avaliações
- ds10 Alcohol PDFDocumento179 páginasds10 Alcohol PDFkatybabyyyAinda não há avaliações
- 10 MindfulnessinEverydayLife PDFDocumento3 páginas10 MindfulnessinEverydayLife PDFkatybabyyyAinda não há avaliações
- VPD Evidence Guide PDFDocumento6 páginasVPD Evidence Guide PDFkatybabyyyAinda não há avaliações
- Healthscope Limited - Housekeeping Cleaner PDFDocumento1 páginaHealthscope Limited - Housekeeping Cleaner PDFkatybabyyyAinda não há avaliações
- CC Map PDFDocumento1 páginaCC Map PDFkatybabyyyAinda não há avaliações
- Sample Cover Letter: No Work ExperienceDocumento3 páginasSample Cover Letter: No Work ExperienceUrien ArancilloAinda não há avaliações
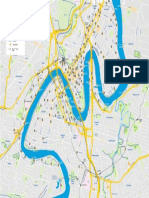
- Loop Brisbanecity PDFDocumento2 páginasLoop Brisbanecity PDFkatybabyyyAinda não há avaliações
- LEFL English Advertisement Dec2014 PDFDocumento1 páginaLEFL English Advertisement Dec2014 PDFkatybabyyyAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Infections and ImmunityDocumento35 páginasInfections and ImmunityDr. Ashish JawarkarAinda não há avaliações
- Prevention Control of Poultry DiseasesDocumento64 páginasPrevention Control of Poultry Diseasessigra100% (3)
- TetraximDocumento5 páginasTetraximkemalahmadAinda não há avaliações
- Cefazolin Ancef Drug CardDocumento2 páginasCefazolin Ancef Drug CardLisaAinda não há avaliações
- DOH Program (EPI)Documento6 páginasDOH Program (EPI)Shaira GumaruAinda não há avaliações
- Final PresentationDocumento43 páginasFinal Presentationapi-608681693Ainda não há avaliações
- MC Question Bank For Quiz 2Documento11 páginasMC Question Bank For Quiz 2necrodamien100% (1)
- Pathogenesis of Type 1 Diabetes MellitusDocumento28 páginasPathogenesis of Type 1 Diabetes MellitusJuan Diego Fernández MurielAinda não há avaliações
- Free Sample Informative SpeechDocumento1 páginaFree Sample Informative SpeechSari Adnin HalimAinda não há avaliações
- Ayurvedic VaccinationDocumento2 páginasAyurvedic VaccinationRadhe GovindaAinda não há avaliações
- Thermostability of Vaccines - WHO - GPV - 98.07 PDFDocumento64 páginasThermostability of Vaccines - WHO - GPV - 98.07 PDFsaveclipAinda não há avaliações
- Pediatric VIVA QuestionsDocumento29 páginasPediatric VIVA Questionsabhivnair93% (14)
- Penicillin Allergy GuidanceDocumento9 páginasPenicillin Allergy Guidancerob burrAinda não há avaliações
- Covid-19 News - Live Updates - The New York TimesDocumento8 páginasCovid-19 News - Live Updates - The New York TimesАртём ЗотинAinda não há avaliações
- Chapter 1 - Performance TaskDocumento18 páginasChapter 1 - Performance Taskmargarita perezAinda não há avaliações
- CH3 - Case 3 Deciding Who Receives The Swine Flu Vaccine (Chapter 3, Page 178)Documento3 páginasCH3 - Case 3 Deciding Who Receives The Swine Flu Vaccine (Chapter 3, Page 178)zoehyhAinda não há avaliações
- Phcist Letter Sept 2006Documento52 páginasPhcist Letter Sept 2006MichelAinda não há avaliações
- Ebola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisDocumento8 páginasEbola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisAuliaZahraAinda não há avaliações
- Awfpc 2022Documento7 páginasAwfpc 2022Jay-p BayonaAinda não há avaliações
- Test - Module 3, Messages 1Documento5 páginasTest - Module 3, Messages 1maya_at100% (3)
- Chapter 19 Practice Multiple ChoiceDocumento8 páginasChapter 19 Practice Multiple Choicekiden300% (1)
- UNICEF DRC - Factsheet On The Situation of Children in DRCDocumento2 páginasUNICEF DRC - Factsheet On The Situation of Children in DRCUnicef RdCongoAinda não há avaliações
- Agglutination Reaction JMHFHSDocumento50 páginasAgglutination Reaction JMHFHSRajkishor YadavAinda não há avaliações
- 8.A Case Report of Rabies With Long Incubation ImporDocumento3 páginas8.A Case Report of Rabies With Long Incubation ImporAndra CristianaAinda não há avaliações
- World Health Organization - Cancer Country Profiles, 2014Documento2 páginasWorld Health Organization - Cancer Country Profiles, 2014Ana BarbosaAinda não há avaliações
- Community-Acquired Pneumonia - CPG 2016Documento26 páginasCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianAinda não há avaliações
- Preventive Medicine: Gypsyamber D'Souza, Amanda DempseyDocumento7 páginasPreventive Medicine: Gypsyamber D'Souza, Amanda DempseyCarla MOAinda não há avaliações
- Feb 09 Formative EMQDocumento10 páginasFeb 09 Formative EMQhallixrapAinda não há avaliações
- DILG MC No. 2021-019Documento8 páginasDILG MC No. 2021-019Roxanne BorlonganAinda não há avaliações
- hlth101 Assignment Presentation Sushma Tandukar 220193829Documento10 páginashlth101 Assignment Presentation Sushma Tandukar 220193829api-526511003Ainda não há avaliações