GRAND
GRAND ROUND
ROUND
Cerebral tuberculoma and
magnetic resonance imaging
A Helmy1
1
NM Antoun2 PJ Hutchinson1
Neurosurgery Unit, Department of Clinical Neurosciences, University of Cambridge, Addenbrookes Hospital,
Cambridge, UK
2
Department of Neuroradiology, Addenbrookes Hospital, Cambridge, UK
Correspondence to: A Helmy. Email: adelhelmy@cantab.net
DECLARATIONS
Competing interests
None declared
This case highlights an unusual presentation of
cerebral tuberculosis (TB) and the associated radiological findings on MRI, including diffusionweighted imaging.
Case report
A 17-year-old Indian man presented with a twomonth history of left-sided headache, morning
Funding
AH is supported by a
joint Medical
Research Council/
Royal College of
Surgeons of England
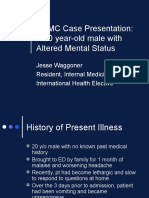
Figure 1
Preoperative MR imaging. a d. Four contiguous slices on T1WI following the injection of gadolinium,
demonstrating the extent of the original lesions. e. A T2WI illustrating the extent of white matter high
signal intensity indicative of cerebral oedema. f. A diffusion-weighted image: it does not show restricted
diffusion (high signal) within the two lesions that would be expected within a liquid abscess
Clinical Research
Training Fellowship
and a Raymond and
Beverly Sackler
Fellowship; PJH is
supported by the
Academy of Medical
Sciences/Health
Foundation
Fellowship
Ethical approval
Written informed
consent to
publication has been
obtained from the
patient or next of kin
Guarantor
PJH
Contributorship
AH conducted the
research and
literature review and
wrote the first draft;
J R Soc Med 2011: 104: 299 301. DOI 10.1258/jrsm.2011.100398
Downloaded from jrs.sagepub.com by guest on September 4, 2016
299
Journal of the Royal Society of Medicine
PJH was responsible
for the clinical
aspects and
overseeing the
paper; NMA was
responsible for
neuroradiology; all
authors contributed
to the final draft of
the paper
Acknowledgements
None
Reviewer
Phillip vanHille
vomiting, visual disturbance and bilateral papilloedema. On direct questioning the patient noted
6 kg of weight loss in the prior six months. On
referral to the acute neurosurgical service MR
imaging was carried out. Following the injection
of gadolinium the lesions enhanced peripherally
on T1-weighted image (T1WI) with multiple
smaller enhancing lesions associated with the
main lesions (Figure 1a d). Two well-defined
(3.5 cm) low signal lesions were demonstrated on
T2-weighted image (T2WI), in the left frontoparietal and right occipital regions, with marked
surrounding oedema (Figure 1e). The diffusionweighted MR sequence did not demonstrate
restricted diffusion (Figure 1f ), as would be
expected of a liquid abscess.1 Chest X-ray was
normal and laboratory findings were as follows: haemoglobin 12.7 g/dl, white cell count 5.9 109/L,
C-reactive protein 20 mg/L. There was no laboratory
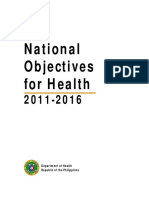
Figure 2
Follow-up MR imaging at three months. a d. The same four slices as
in Figures 1a d on T1WI following the injection of gadolinium. The
operated (left parietal) lesion has completed disappeared. The
non-operated (right occipital) lesion has significantly decreased in
size reflecting a good response to medical therapy
300
J R Soc Med 2011: 104: 299 301. DOI 10.1258/jrsm.2011.100398
or clinical evidence of an immunocompromised
state.
In view of the mass effect caused by the left
fronto-parietal lesion and the uncertain diagnosis
the patient underwent an emergent image-guided
craniotomy and excision of the left-sided lesion.
At craniotomy a hard, well-circumscribed lesion
was identified with a similar colour to normal
white matter. Histology confirmed cerebral tuberculoma, as evidenced by granuloma formation
and a single acid-fast bacillus. Subsequent chest
CT identified pulmonary TB. The patient commenced anti-tuberculous triple therapy with
Rifater, moxifloxacin, pyridoxine and dexamethasone.2 At three-month follow-up his presenting
symptoms and papilloedema had resolved and
he was gaining weight. Repeat MR imaging at
this point demonstrated complete surgical excision of the parietal lesion and a reduction in the
size of the occipital lesion with reduced oedema
suggestive of a response to pharmacological
therapy (Figure 2).
Discussion
The global incidence of TB is increasing, even
in the immunocompetent population.3 Central
nervous system TB is most common in those
aged below 20 years (60 70% of cases), and coexistent extra-neural TB is only reported in 50%
cases, as in this case.4 Central nervous system TB
most commonly takes the form of meningeal
disease (leptomeningitis or more rarely pachymeningitis) as well as the parenchymal disease
described here (tuberculous granuloma [tuberculoma], tuberculous abscess, focal cerebritis and
allergic tuberculous encephalopathy)5. The
most common clinical presentation of a tuberculoma is headache, signs of intracranial hypertension, focal neurological deficit and seizure.
Tuberculous meningitis is characterized radiologically by the triad of basal meningeal
enhancement, hydrocephalus and cerebral infarction, though a range of other features are
common.5 Cerebral tuberculomas are most
common at the cortico-medullary junction,
especially in the frontal and parietal lobes, as
they are often the result of haematogenous
spread as part of miliary TB.6 Diffusion-weighted
MR is a useful adjunct in abscesses as the central
Downloaded from jrs.sagepub.com by guest on September 4, 2016
Cerebral tuberculoma and magnetic resonance imaging
portion of an abscess will demonstrate restricted
diffusion however this is not the case in a true
tuberculoma.5
Follow-up imaging following appropriate antituberculous pharmacotherapy allows the response
to therapy to be gauged, with the degree of contrast enhancement and surrounding oedema
related to the activity within the tuberculoma.7 A
high index of clinical suspicion is required to
allow rapid diagnosis of this condition in order
to institute rapid treatment and avoid potentially
serious neurological sequelae.
References
1
Lai PH, Hsu SS, Lo YK, Ding SW. Role of diffusion-weighted
imaging and proton MR spectroscopy in distinguishing
between pyogenic brain abscess and necrotic brain tumor.
Acta Neurol Taiwan 2004;13:107 13
Thwaites G, Fisher M, Hemingway C, Scott G, Solomon T,
Innes J. British Infection Society guidelines for the
diagnosis and treatment of tuberculosis of the central
nervous system in adults and children. J Infect
2009;59:167 87
Dye C, Lonnroth K, Jaramillo E, Williams BG, Raviglione
M. Trends in tuberculosis incidence and their determinants
in 134 countries. Bull World Health Organ 2009;87:
683 91
Kumar R, Jain R, Kaur A, Chhabra DK. Brain stem
tuberculosis in children. Br J Neurosurg 2000;14:
356 61
Bernaerts A, Vanhoenacker FM, Parizel PM, et al.
Tuberculosis of the central nervous system: overview
of neuroradiological findings. Eur Radiol 2003;13:
1876 90
Gupta RK, Kohli A, Gaur V, Lal JH, Kishore J.
MRI of the brain in patients with miliary pulmonary
tuberculosis without symptoms or signs of central
nervous system involvement. Neuroradiology
1997;39:699 704
McGuinness F. Clinical Imaging in non-pulmonary tuberculosis.
New York, NY: Springer, 2000
J R Soc Med 2011: 104: 299 301. DOI 10.1258/jrsm.2011.100398
Downloaded from jrs.sagepub.com by guest on September 4, 2016
301
Você também pode gostar
- Chapter 19Documento29 páginasChapter 19Carmela Laraya Alayon100% (3)
- Community HealthDocumento52 páginasCommunity Healthshangsyndrome100% (2)
- Class Notes 1 Pharmaceutical Supply Chain ManagementDocumento13 páginasClass Notes 1 Pharmaceutical Supply Chain ManagementNdatasha PambweAinda não há avaliações
- Self Administered Exam 4Documento31 páginasSelf Administered Exam 4priyarajan007100% (4)
- Health Quarter 3 - Module Health Trends, Issues and Concerns (Global Level)Documento22 páginasHealth Quarter 3 - Module Health Trends, Issues and Concerns (Global Level)Mary Cris GoAinda não há avaliações
- Child With Respiratory DisorderDocumento48 páginasChild With Respiratory DisorderEmjay JapitanaAinda não há avaliações
- Hospital Pharmacy LabDocumento179 páginasHospital Pharmacy LabJohn Carlo Cabueñas RagmaAinda não há avaliações
- Infection ControlDocumento21 páginasInfection ControlAwaisAinda não há avaliações
- Anti TB DrugsDocumento46 páginasAnti TB Drugs88AKKAinda não há avaliações
- Jurnal MRKHDocumento6 páginasJurnal MRKHTitii Tri'b WinarsihAinda não há avaliações
- National Health ProgrammesDocumento12 páginasNational Health ProgrammesRAJU100% (2)
- Lee 2007Documento6 páginasLee 2007Luis PerezAinda não há avaliações
- Radio Logical Finding PCNSLDocumento12 páginasRadio Logical Finding PCNSLKhushalchand KanjiAinda não há avaliações
- 104.full AdemDocumento6 páginas104.full AdemayubahriAinda não há avaliações
- Hon 2005Documento2 páginasHon 2005Andana TrisaviAinda não há avaliações
- Radiologic and Clinical Findings in Tuberculous MeningitisDocumento6 páginasRadiologic and Clinical Findings in Tuberculous MeningitisAustine OsaweAinda não há avaliações
- MR Spectroscopy-Aided Differentiation: "Giant" Extra-Axial Tuberculoma Masquerading As MeningiomaDocumento3 páginasMR Spectroscopy-Aided Differentiation: "Giant" Extra-Axial Tuberculoma Masquerading As Meningiomaselvie87Ainda não há avaliações
- Síndrome de Gradenigo #2Documento5 páginasSíndrome de Gradenigo #2Arcel De Luca G.Ainda não há avaliações
- Mediastinal Tuberculous Lymphadenitis Presenting With Insidious Back Pain in A Male Adult: A Case Report and Review of The LiteratureDocumento7 páginasMediastinal Tuberculous Lymphadenitis Presenting With Insidious Back Pain in A Male Adult: A Case Report and Review of The Literaturez9tpwgb5nwAinda não há avaliações
- Meningoencephalitis and New Onset of Seizures in A Patient With Normal Brain CT and Multiple Lesions On MRIDocumento3 páginasMeningoencephalitis and New Onset of Seizures in A Patient With Normal Brain CT and Multiple Lesions On MRITryas YulithaAinda não há avaliações
- Apik Case of The Month 09-2012Documento9 páginasApik Case of The Month 09-2012Naily Nuzulur RohmahAinda não há avaliações
- GM 04015Documento6 páginasGM 04015Ikhsan FebriansyahAinda não há avaliações
- Brandsma 2001Documento4 páginasBrandsma 2001VoltajeAinda não há avaliações
- Follow UpDocumento6 páginasFollow UpWinda HaeriyokoAinda não há avaliações
- SSP 1Documento5 páginasSSP 1YanAinda não há avaliações
- A Case Report of Clonal EBV-like Memory CD4.sup.+ T Cell Activation in Fatal Checkpoint Inhibitor-Induced EncephalitisDocumento24 páginasA Case Report of Clonal EBV-like Memory CD4.sup.+ T Cell Activation in Fatal Checkpoint Inhibitor-Induced Encephalitismikeb92556Ainda não há avaliações
- Case Report: A Rare Case of Central Nervous System TuberculosisDocumento6 páginasCase Report: A Rare Case of Central Nervous System TuberculosislittlecandiesAinda não há avaliações
- Extracranial Metastases of Anaplastic Meningioma: Case ReportDocumento6 páginasExtracranial Metastases of Anaplastic Meningioma: Case ReportRizky AdriansahAinda não há avaliações
- J Neurol Neurosurg Psychiatry 2005 Vanopdenbosch 1017 8Documento3 páginasJ Neurol Neurosurg Psychiatry 2005 Vanopdenbosch 1017 8afiwahyuAinda não há avaliações
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Documento9 páginasP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)zano_adamAinda não há avaliações
- Tuberculous Meningitis: Basal Cistern Enhancement Pattern On CT ImagingDocumento9 páginasTuberculous Meningitis: Basal Cistern Enhancement Pattern On CT ImagingDeei RizalAinda não há avaliações
- Central Variant PRESDocumento5 páginasCentral Variant PRESAbdul AzeezAinda não há avaliações
- Clinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old ManDocumento8 páginasClinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old MansamuelAinda não há avaliações
- E110 FullDocumento2 páginasE110 FullLuther ThengAinda não há avaliações
- KCMC Case Presentation: A 20 Year-Old Male With Altered Mental StatusDocumento20 páginasKCMC Case Presentation: A 20 Year-Old Male With Altered Mental StatusJessica GarletsAinda não há avaliações
- Adem LikeDocumento4 páginasAdem LikeRodrigo AriasAinda não há avaliações
- Tolosa-Hunt Syndrome in Double-Hit Lymphoma: Case Reports in Oncological Medicine March 2015Documento6 páginasTolosa-Hunt Syndrome in Double-Hit Lymphoma: Case Reports in Oncological Medicine March 2015Elisabeth TikalakaAinda não há avaliações
- Neuroimaging in The Brain in HIV-1-Infected PatientsDocumento25 páginasNeuroimaging in The Brain in HIV-1-Infected PatientsYanina Pérez de VillarrealAinda não há avaliações
- SM Pediatric Balolike 10072 - 2022 - Article - 6396Documento3 páginasSM Pediatric Balolike 10072 - 2022 - Article - 6396Tunde CsepanyAinda não há avaliações
- Fulltext Ajo v2 Id1026Documento3 páginasFulltext Ajo v2 Id1026Lavenia Ellein MokiwangAinda não há avaliações
- AbscessDocumento12 páginasAbscesslittlecandiesAinda não há avaliações
- Dermatomyositis and Undifferentiated Nasopharyngeal Carcinoma. A Rare Presentation of A Rare MalignancyDocumento4 páginasDermatomyositis and Undifferentiated Nasopharyngeal Carcinoma. A Rare Presentation of A Rare MalignancyasclepiuspdfsAinda não há avaliações
- 10.1007@s11060 004 3390 7Documento9 páginas10.1007@s11060 004 3390 7AlejitaplafuenteAinda não há avaliações
- Cerebral Toxoplasmosis With Immunocompromised Tugas PKBDocumento12 páginasCerebral Toxoplasmosis With Immunocompromised Tugas PKBApriliaAinda não há avaliações
- MRI Spectrum of CNS Tuberculosis: Pictorial CmeDocumento8 páginasMRI Spectrum of CNS Tuberculosis: Pictorial CmeAs AsAinda não há avaliações
- Immune Reconstitution Inflammatory Syndrome and Cerebral ToxoplasmosisDocumento2 páginasImmune Reconstitution Inflammatory Syndrome and Cerebral ToxoplasmosisFirda PotterAinda não há avaliações
- tmpBAE8 TMPDocumento6 páginastmpBAE8 TMPFrontiersAinda não há avaliações
- Narrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaDocumento6 páginasNarrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaJavier Perez ManriquezAinda não há avaliações
- Case ReportDocumento3 páginasCase ReportNeilavery WindaAinda não há avaliações
- Respiratory Medicine Case Reports: Regina Monteiro, José Carlos Carneiro, Claúdia Costa, Raquel DuarteDocumento4 páginasRespiratory Medicine Case Reports: Regina Monteiro, José Carlos Carneiro, Claúdia Costa, Raquel DuarterezaAinda não há avaliações
- JurnalDocumento9 páginasJurnalMelita Amalia AyubaAinda não há avaliações
- Disseminated Miliary Cerebral Candidiasis: Candida Albicans Is The Most Common Nos-C AlbicansDocumento4 páginasDisseminated Miliary Cerebral Candidiasis: Candida Albicans Is The Most Common Nos-C Albicansdrian pamungkasAinda não há avaliações
- Medi 101 E28665Documento5 páginasMedi 101 E28665S Francisco MotAinda não há avaliações
- Outcomes of Tuberculous Meningitis in ChildrenDocumento31 páginasOutcomes of Tuberculous Meningitis in ChildrenDelphine DedelAinda não há avaliações
- Autoimmune Inner Ear Disease in A Melanoma Patient Treated With PembrolizumabDocumento6 páginasAutoimmune Inner Ear Disease in A Melanoma Patient Treated With PembrolizumabIndRa KaBhuomAinda não há avaliações
- Complications of Radiotherapy and Radiosurgery inDocumento7 páginasComplications of Radiotherapy and Radiosurgery inzn69h45hn4Ainda não há avaliações
- SC 201543Documento7 páginasSC 201543esinsubozatliAinda não há avaliações
- Radiculopatia CervicalDocumento8 páginasRadiculopatia CervicalFACIVERIAinda não há avaliações
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDocumento5 páginasCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarAinda não há avaliações
- Paravertebral AbscessDocumento3 páginasParavertebral AbscessAlam MartadipuraAinda não há avaliações
- Case Report: Intracranial Multiple Germ Cell Tumors: A Case Report and Review of LiteratureDocumento6 páginasCase Report: Intracranial Multiple Germ Cell Tumors: A Case Report and Review of Literaturearcobaleno589Ainda não há avaliações
- Current Epidemiological Trends of Brain Abscess: A Clinicopathological StudyDocumento9 páginasCurrent Epidemiological Trends of Brain Abscess: A Clinicopathological StudyNur Fadhilah KusnadiAinda não há avaliações
- Case Report: Tuberculous Spondylitis: A Report of Different Clinical Scenarios and Literature UpdateDocumento5 páginasCase Report: Tuberculous Spondylitis: A Report of Different Clinical Scenarios and Literature UpdatepuaanAinda não há avaliações
- Tuberculous Spondylitis PDFDocumento5 páginasTuberculous Spondylitis PDFpuaanAinda não há avaliações
- A Rare Case of Space Occupying Lesion of Brainstem in An Elderly Male PatientDocumento3 páginasA Rare Case of Space Occupying Lesion of Brainstem in An Elderly Male PatientInternational Journal of Clinical and Biomedical Research (IJCBR)Ainda não há avaliações
- 72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientDocumento7 páginas72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientFaras ArinalAinda não há avaliações
- T-Cell/histiocyte-Rich Large B-Cell Lymphoma Presenting As A Primary Central Nervous System Lymphoma.Documento3 páginasT-Cell/histiocyte-Rich Large B-Cell Lymphoma Presenting As A Primary Central Nervous System Lymphoma.pancholarpancholarAinda não há avaliações
- Cluster Headache: When To Worry? Two Case ReportsDocumento5 páginasCluster Headache: When To Worry? Two Case ReportsNamira AmmarinAinda não há avaliações
- NIH Public Access: Author ManuscriptDocumento6 páginasNIH Public Access: Author ManuscriptAnonymous G20oAbl6p8Ainda não há avaliações
- DDMS 20230303-27972-QiqbxtDocumento7 páginasDDMS 20230303-27972-QiqbxtjournalijoifmAinda não há avaliações
- Multiple Sclerosis and CNS Inflammatory DisordersNo EverandMultiple Sclerosis and CNS Inflammatory DisordersLawrence M. SamkoffAinda não há avaliações
- Tuberculoma OF THE Brain (Revisited)Documento7 páginasTuberculoma OF THE Brain (Revisited)Nyoman SuryaAinda não há avaliações
- Disruptive Mood Dysregulation DisorderDocumento13 páginasDisruptive Mood Dysregulation DisorderNyoman SuryaAinda não há avaliações
- Fnins-Sex Hormon NeuroDocumento20 páginasFnins-Sex Hormon NeuroNyoman SuryaAinda não há avaliações
- Itp InyoDocumento1 páginaItp InyoNyoman SuryaAinda não há avaliações
- Defenisi PDFDocumento2 páginasDefenisi PDFNyoman SuryaAinda não há avaliações
- Analisis Strategi Pemasaran Peternakan Ayam CV Intan Jaya Abadi SukabumiDocumento8 páginasAnalisis Strategi Pemasaran Peternakan Ayam CV Intan Jaya Abadi SukabumiNyoman SuryaAinda não há avaliações
- Ginsen No KazeDocumento1 páginaGinsen No KazeNyoman SuryaAinda não há avaliações
- Uninstall - Ishikawa ChiakiDocumento2 páginasUninstall - Ishikawa ChiakiNyoman SuryaAinda não há avaliações
- Patogenesis Virus DiareDocumento1 páginaPatogenesis Virus DiareNyoman SuryaAinda não há avaliações
- DokpenDocumento18 páginasDokpenNyoman SuryaAinda não há avaliações
- Headaches For EducatorsDocumento38 páginasHeadaches For EducatorsRidzky FirmansyahAinda não há avaliações
- LicenseDocumento4 páginasLicenseObby ObediAinda não há avaliações
- Ameagari No Niji Mo Rin To Saita Hana MoDocumento2 páginasAmeagari No Niji Mo Rin To Saita Hana MoNyoman SuryaAinda não há avaliações
- YUI - My SoulDocumento2 páginasYUI - My SoulNyoman SuryaAinda não há avaliações
- Noisycell - InnocentDocumento1 páginaNoisycell - InnocentNyoman SuryaAinda não há avaliações
- DAYS of DASHDocumento2 páginasDAYS of DASHNyoman SuryaAinda não há avaliações
- DAYS of DASHDocumento2 páginasDAYS of DASHNyoman SuryaAinda não há avaliações
- Minami Kuribayashi - ZeroDocumento1 páginaMinami Kuribayashi - ZeroNyoman SuryaAinda não há avaliações
- Brain Metastases From Breast Cancer - Management Approach Wadasadawala T, Gupta S, Bagul V, Patil N - J Can Res TherDocumento10 páginasBrain Metastases From Breast Cancer - Management Approach Wadasadawala T, Gupta S, Bagul V, Patil N - J Can Res TherNyoman SuryaAinda não há avaliações
- Gus156 Slide Blok Genitourinary SystemDocumento46 páginasGus156 Slide Blok Genitourinary Systempetje23Ainda não há avaliações
- A Naoidhean Bhig Cluinn Mo GhuthDocumento1 páginaA Naoidhean Bhig Cluinn Mo GhuthNyoman SuryaAinda não há avaliações
- P ('t':'3', 'I':'1920701825') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Documento4 páginasP ('t':'3', 'I':'1920701825') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Nyoman SuryaAinda não há avaliações
- Tugas Adjective Arnia PoerbasariDocumento3 páginasTugas Adjective Arnia PoerbasariNyoman SuryaAinda não há avaliações
- NvwinstrfhjjggyeamconfigDocumento2 páginasNvwinstrfhjjggyeamconfigFlorin CirlanAinda não há avaliações
- 10 Small Ways To Gain Respect As A LeaderDocumento2 páginas10 Small Ways To Gain Respect As A LeaderNyoman SuryaAinda não há avaliações
- Jurnal Riset Gizi: p-ISSN: e-ISSNDocumento5 páginasJurnal Riset Gizi: p-ISSN: e-ISSNRia HarmonisAinda não há avaliações
- Noh2016 PDFDocumento149 páginasNoh2016 PDFSef MartinezAinda não há avaliações
- Jurding TBDocumento26 páginasJurding TBRaja Ahmad Rusdan MusyawirAinda não há avaliações
- Exploring The Limitations of BCG VaccineDocumento7 páginasExploring The Limitations of BCG Vaccinenajdah_220754970Ainda não há avaliações
- TB Dots Program 11Documento28 páginasTB Dots Program 11Mark SamonteAinda não há avaliações
- Infectious Diseases: A Case of Tuberculosis Verrucosa Cutis in Brazil Undiagnosed For 15 YearsDocumento3 páginasInfectious Diseases: A Case of Tuberculosis Verrucosa Cutis in Brazil Undiagnosed For 15 YearsAnthony SetiawanAinda não há avaliações
- CHN Ebr 1Documento2 páginasCHN Ebr 1nissieAinda não há avaliações
- Module 3. Study GuideDocumento5 páginasModule 3. Study Guidekaren solibaAinda não há avaliações
- TB MDR Ruth Putri-1510015071Documento16 páginasTB MDR Ruth Putri-1510015071Elizabeth SagalaAinda não há avaliações
- MusicDocumento9 páginasMusicJerico Villa MaglasangAinda não há avaliações
- Respiratory Medicine Case Reports: Regina Monteiro, José Carlos Carneiro, Claúdia Costa, Raquel DuarteDocumento4 páginasRespiratory Medicine Case Reports: Regina Monteiro, José Carlos Carneiro, Claúdia Costa, Raquel DuarterezaAinda não há avaliações
- The PhilCAT Certification Self-Assessment and Survey ToolDocumento25 páginasThe PhilCAT Certification Self-Assessment and Survey ToolEivenn PanerioAinda não há avaliações
- Third Quarter Module 1: Global Health Initiatives (Week 1)Documento18 páginasThird Quarter Module 1: Global Health Initiatives (Week 1)Rhian Velasquez100% (1)
- List Pasien 24-26 November 2023...Documento2 páginasList Pasien 24-26 November 2023...Rasi sallangAinda não há avaliações
- Microbiology and Parasitology Summary and ChartsDocumento54 páginasMicrobiology and Parasitology Summary and Chartssciencetopic4Ainda não há avaliações
- Evaluasi Pelaksanaan Program Penanggulangan Tuberkulosis Paru (P2Tb) Di Puskesmas Bandarharjo Kota SemarangDocumento12 páginasEvaluasi Pelaksanaan Program Penanggulangan Tuberkulosis Paru (P2Tb) Di Puskesmas Bandarharjo Kota Semarangasih wulandariAinda não há avaliações
- TB Chapter17Documento19 páginasTB Chapter17Avery Wiese100% (2)
- Pregnancy and TBDocumento24 páginasPregnancy and TBRoza MaulindraAinda não há avaliações
- Zoonotic TB Factsheet 2Documento2 páginasZoonotic TB Factsheet 2nicol avilaAinda não há avaliações
- Quiz BSN 4Documento1 páginaQuiz BSN 4Mae Marie Jambaro-TuaAinda não há avaliações