Você também pode gostar
- Penentuan Tafsiran Berat JaninDocumento5 páginasPenentuan Tafsiran Berat JaninNenny Yoanitha Djala100% (1)
- Cover Program Kerja Obgyn 2017Documento1 páginaCover Program Kerja Obgyn 2017Nenny Yoanitha DjalaAinda não há avaliações
- How To Explore After Forceps ExtractionDocumento7 páginasHow To Explore After Forceps ExtractionNenny Yoanitha DjalaAinda não há avaliações
- Reichman 2014Documento5 páginasReichman 2014Nenny Yoanitha DjalaAinda não há avaliações
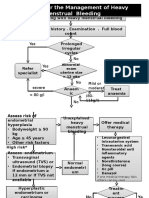
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 páginasAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaAinda não há avaliações
- Penentuan Tafsiran Berat JaninDocumento5 páginasPenentuan Tafsiran Berat JaninNenny Yoanitha DjalaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- 209 (8) 6Documento1 página209 (8) 6Rajesh DmAinda não há avaliações
- Daftar Harga Obat ApotekDocumento7 páginasDaftar Harga Obat ApoteksalmaegaAinda não há avaliações
- Heart Block and Their Best Treatment in Homeopathy - Bashir Mahmud ElliasDocumento13 páginasHeart Block and Their Best Treatment in Homeopathy - Bashir Mahmud ElliasBashir Mahmud Ellias50% (2)
- Master Tecniques TornozeloDocumento834 páginasMaster Tecniques TornozeloOrtopedia FabioAinda não há avaliações
- ME 4 - Acute and Post Acute COVID-19 Neurological Syndrome-How To Manage - Dr. Kartika Maharani, SP.S (K) - 1Documento31 páginasME 4 - Acute and Post Acute COVID-19 Neurological Syndrome-How To Manage - Dr. Kartika Maharani, SP.S (K) - 1winnerfromparisAinda não há avaliações
- Uterine Leiomyomas (Fibroids) - Epidemiology, Clinical Features, Diagnosis, and Natural History - UpToDateDocumento48 páginasUterine Leiomyomas (Fibroids) - Epidemiology, Clinical Features, Diagnosis, and Natural History - UpToDateRuben Orduño RizoAinda não há avaliações
- Îeéuwûéaéié Uréékéï: (Diseases of Tongue)Documento87 páginasÎeéuwûéaéié Uréékéï: (Diseases of Tongue)Pranit Patil100% (1)
- Review Article: Inhaled Therapy in Respiratory Disease: The Complex Interplay of Pulmonary Kinetic ProcessesDocumento12 páginasReview Article: Inhaled Therapy in Respiratory Disease: The Complex Interplay of Pulmonary Kinetic ProcessesliadiafaridaAinda não há avaliações
- Urdaneta City University Graduate School UrdanetaDocumento13 páginasUrdaneta City University Graduate School UrdanetaMa Theresa PunoAinda não há avaliações
- Neuropathology: Stroke With Kartik Rangaraj MDDocumento37 páginasNeuropathology: Stroke With Kartik Rangaraj MDAbdi fatah ali1Ainda não há avaliações
- Seminar On Shock: IndexDocumento37 páginasSeminar On Shock: IndexGayathri R100% (1)
- MCQ Final 2014Documento19 páginasMCQ Final 2014JohnSon100% (1)
- Piperacillin TazobactamDocumento2 páginasPiperacillin TazobactamAnonymous43% (7)
- Management of Acne Scarring, Part II: A Comparative Review of Non-Laser-Based, Minimally Invasive ApproachesDocumento10 páginasManagement of Acne Scarring, Part II: A Comparative Review of Non-Laser-Based, Minimally Invasive ApproachesShintaAinda não há avaliações
- BronchiectasisDocumento30 páginasBronchiectasisMark Gizle PapagayoAinda não há avaliações
- Med Surg (Oncology)Documento169 páginasMed Surg (Oncology)DardarConstantinoAinda não há avaliações
- Paediatrics: Final Exam National Board of Examinations December 2011Documento4 páginasPaediatrics: Final Exam National Board of Examinations December 2011AlolikaAinda não há avaliações
- Children Complete QSTDocumento1 páginaChildren Complete QSTHoda AtwaAinda não há avaliações
- Serosal Appendicitis: Incidence, Causes and Clinical SignificanceDocumento3 páginasSerosal Appendicitis: Incidence, Causes and Clinical SignificancenaufalrosarAinda não há avaliações
- A Study On Level of Mental Health Problems of AdolescentDocumento3 páginasA Study On Level of Mental Health Problems of AdolescentEditor IJTSRDAinda não há avaliações
- Principle:: Sample Considerations and Special ProceduresDocumento97 páginasPrinciple:: Sample Considerations and Special Proceduresjustine anchetaAinda não há avaliações
- Freedom Is Therapeutic Prof John FootDocumento2 páginasFreedom Is Therapeutic Prof John FootAna WongAinda não há avaliações
- Vertigo and Balance TX ArticleDocumento7 páginasVertigo and Balance TX Articleapi-262531856Ainda não há avaliações
- Advanced Drug Delivery Reviews: Sadaf Aghevlian, Amanda J. Boyle, Raymond M. ReillyDocumento17 páginasAdvanced Drug Delivery Reviews: Sadaf Aghevlian, Amanda J. Boyle, Raymond M. ReillyKamila MartinAinda não há avaliações
- Preview Pages of A Practical Guide On Pharmacovigilance For BeginnersDocumento19 páginasPreview Pages of A Practical Guide On Pharmacovigilance For BeginnersdrgunasakaranAinda não há avaliações
- The Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesDocumento9 páginasThe Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesimuhammadfahmiAinda não há avaliações
- Total Intravenous Anaesthesia (TIVA)Documento4 páginasTotal Intravenous Anaesthesia (TIVA)Doby Oktovian Alfarizi100% (1)
- Caring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyDocumento34 páginasCaring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyRubinaAinda não há avaliações
- BSC in Neonatal NursingDocumento14 páginasBSC in Neonatal NursingsmsmdsdsffAinda não há avaliações
- RBC Disorder BcqsDocumento68 páginasRBC Disorder BcqsMukhtiar AhmedAinda não há avaliações