Você também pode gostar
- Test Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiDocumento479 páginasTest Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiBetsy Brown Byersmith89% (133)
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsAinda não há avaliações
- CA-1032 RevisedDocumento9 páginasCA-1032 RevisedSandy Zertuche50% (2)
- Claim Form Dd2642Documento4 páginasClaim Form Dd2642Adina BusteaAinda não há avaliações
- Edi FormDocumento2 páginasEdi Formapi-240084111Ainda não há avaliações
- Newman's Medical Billing and Coding Technicians Study GuideNo EverandNewman's Medical Billing and Coding Technicians Study GuideAinda não há avaliações
- Medical Coding: a QuickStudy Laminated Reference GuideNo EverandMedical Coding: a QuickStudy Laminated Reference GuideAinda não há avaliações
- Case StudyDocumento49 páginasCase StudyLennie Marie B Pelaez100% (1)
- C I Care Badge CardsDocumento1 páginaC I Care Badge CardsMai MaiAinda não há avaliações
- Poultry Diseases and Their TreatmentDocumento159 páginasPoultry Diseases and Their TreatmentAbubakar Tahir Ramay67% (12)
- Workers CompensationDocumento12 páginasWorkers Compensationapi-341253302Ainda não há avaliações
- Dental Expense Claim: SECTION 1: To Be Completed by EmployeeDocumento6 páginasDental Expense Claim: SECTION 1: To Be Completed by EmployeeandryAinda não há avaliações
- Delta Dental: P.O Box 997330 Customer Service 888-335Documento1 páginaDelta Dental: P.O Box 997330 Customer Service 888-335yopinomleniAinda não há avaliações
- 2 Claim Form A - Other Than PA and TravelDocumento3 páginas2 Claim Form A - Other Than PA and TravelEkta ChauhanAinda não há avaliações
- Kr-Insurance Comparison ChartDocumento14 páginasKr-Insurance Comparison Chartapi-279983720Ainda não há avaliações
- Standard Claim Form InsuredDocumento2 páginasStandard Claim Form InsuredknsaravanaAinda não há avaliações
- Member Dental Claim Form: Mark All Applicable Boxes)Documento4 páginasMember Dental Claim Form: Mark All Applicable Boxes)TreyAinda não há avaliações
- Health Insurance Claim Form: Please Do Not Staple in This AreaDocumento2 páginasHealth Insurance Claim Form: Please Do Not Staple in This Areatmnunes0419Ainda não há avaliações
- NAS - Reimbursement Claim FormDocumento2 páginasNAS - Reimbursement Claim FormPIANGO40% (5)
- NTUC Claim FormDocumento5 páginasNTUC Claim FormHihiAinda não há avaliações
- Texas Employees Group Benefits Program (GBP) Supplemental Information Form For EmployeesDocumento2 páginasTexas Employees Group Benefits Program (GBP) Supplemental Information Form For EmployeesBhargav Teja NukalaAinda não há avaliações
- Medical ClaimDocumento3 páginasMedical Claimpipul36Ainda não há avaliações
- Part A - To Be Completed by Applicant (Or Authorized Third Party Representative)Documento2 páginasPart A - To Be Completed by Applicant (Or Authorized Third Party Representative)malcolm grantAinda não há avaliações
- Health Suraksha Claim FormDocumento2 páginasHealth Suraksha Claim FormAnna MalaiAinda não há avaliações
- Phil Health ClaimForm GuidelinesDocumento7 páginasPhil Health ClaimForm GuidelinesFerdinand CordovizAinda não há avaliações
- Medical Claim Reimbursement Form EnglishDocumento2 páginasMedical Claim Reimbursement Form EnglishHananAhmedAinda não há avaliações
- Claim Intimation Form Insurance 0Documento2 páginasClaim Intimation Form Insurance 0Vishal SankheAinda não há avaliações
- Singapore Dental Claim Form Interactive M003 60E 010115Documento5 páginasSingapore Dental Claim Form Interactive M003 60E 010115Nazim SalehAinda não há avaliações
- IRDA Reimbursement Claim Form - InsuredDocumento2 páginasIRDA Reimbursement Claim Form - InsuredSoham BanerjeeAinda não há avaliações
- Nic Claim FormDocumento2 páginasNic Claim FormGopalKrishnaAinda não há avaliações
- Metlife Dental Claim FormDocumento4 páginasMetlife Dental Claim FormcoresourceAinda não há avaliações
- Cms Form1500Documento2 páginasCms Form1500jhite01Ainda não há avaliações
- 1.reimbursement Claim FormDocumento3 páginas1.reimbursement Claim FormVijiAinda não há avaliações
- New Claim Form TTK TPADocumento2 páginasNew Claim Form TTK TPAAbhijit SawantAinda não há avaliações
- Claim Form Dhs ReimbursementDocumento4 páginasClaim Form Dhs Reimbursementyyateen0% (1)
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocumento4 páginasClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Auser4timepass6237Ainda não há avaliações
- Claim FormDocumento2 páginasClaim FormdtoxidAinda não há avaliações
- Ericsson Claim Form PDFDocumento2 páginasEricsson Claim Form PDFlovingsayrus100% (1)
- Easy Health Insurance Claim FormDocumento8 páginasEasy Health Insurance Claim FormDiwakar NaiduAinda não há avaliações
- Claim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Documento4 páginasClaim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Boby GanaAinda não há avaliações
- Kenneth Blau, M.D.'S Connecticut Licensure ApplicationsDocumento30 páginasKenneth Blau, M.D.'S Connecticut Licensure Applicationscrush2482Ainda não há avaliações
- Claimant Statement Form Death Claim 2Documento3 páginasClaimant Statement Form Death Claim 2Anitha AnuAinda não há avaliações
- Letterhead of Referring ESI Hospital (P-I) : Referral Form (Permission Letter)Documento8 páginasLetterhead of Referring ESI Hospital (P-I) : Referral Form (Permission Letter)Arpit SharmaAinda não há avaliações
- Appointment of Rep Form 1Documento2 páginasAppointment of Rep Form 1Kyle Wendl PaatAinda não há avaliações
- Family Floater Claim FormDocumento4 páginasFamily Floater Claim FormSAMAinda não há avaliações
- Registering As A Dentist With The General Dental Council (EU/EEA/Switzerland)Documento14 páginasRegistering As A Dentist With The General Dental Council (EU/EEA/Switzerland)Georgia SkopelitiAinda não há avaliações
- Health Claim Form - CholamandalamDocumento4 páginasHealth Claim Form - Cholamandalamsomasreekanth422Ainda não há avaliações
- Hospitalisation Claim FormsDocumento6 páginasHospitalisation Claim FormspritamAinda não há avaliações
- Med 1Documento4 páginasMed 1api-259279833Ainda não há avaliações
- Ohip ApplicationDocumento4 páginasOhip Applicationapi-310747685Ainda não há avaliações
- Premera Claim FormDocumento1 páginaPremera Claim FormManoj GuptaAinda não há avaliações
- Registering As A Dentist With The General Dental Council (Overseas Qualified)Documento18 páginasRegistering As A Dentist With The General Dental Council (Overseas Qualified)zahra seraj0% (1)
- G 740sDocumento2 páginasG 740sapi-167123914Ainda não há avaliações
- MediPrime Claim FormDocumento8 páginasMediPrime Claim Formrahul0105100% (1)
- GMHP Claim Form - Online PDFDocumento4 páginasGMHP Claim Form - Online PDFSalem AmraneAinda não há avaliações
- ICNCDRS Blindness Registry FormDocumento4 páginasICNCDRS Blindness Registry FormAprilAngeliRobleAinda não há avaliações
- Common PSURIClaim FormDocumento5 páginasCommon PSURIClaim FormSandeep PawarAinda não há avaliações
- Newman's Billing and Coding Technicians Study GuideNo EverandNewman's Billing and Coding Technicians Study GuideNota: 4.5 de 5 estrelas4.5/5 (2)
- Cross-Training: The Medical Assistant WorkbookNo EverandCross-Training: The Medical Assistant WorkbookAinda não há avaliações
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsAinda não há avaliações
- Textbook of Urgent Care Management: Chapter 21, Employment Contracts and CompensationNo EverandTextbook of Urgent Care Management: Chapter 21, Employment Contracts and CompensationAinda não há avaliações
- Wiley Tax Preparer: A Guide to Form 1040No EverandWiley Tax Preparer: A Guide to Form 1040Ainda não há avaliações
- Cleveland Clinic and Hebrew University: A Virtual Partnership To Redefine Nanotechnology?Documento10 páginasCleveland Clinic and Hebrew University: A Virtual Partnership To Redefine Nanotechnology?kirtiAinda não há avaliações
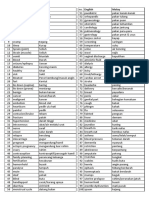
- Medic Term English MalayDocumento1 páginaMedic Term English MalaySyamimi SuhaimiAinda não há avaliações
- Answers To Virology MCQ Paper 1Documento8 páginasAnswers To Virology MCQ Paper 1Idrissa ContehAinda não há avaliações
- Summary of Vaccine Procurement, Donation Processing, and Approval (By The National Government)Documento6 páginasSummary of Vaccine Procurement, Donation Processing, and Approval (By The National Government)December CoolAinda não há avaliações
- Indications Dose Duration Administration Stability Warning & PrecautionsDocumento2 páginasIndications Dose Duration Administration Stability Warning & PrecautionsFatma HasanAinda não há avaliações
- Chemical Biology: Semester - Iii and Vii 2017-18Documento12 páginasChemical Biology: Semester - Iii and Vii 2017-18Yogesh ShekhawatAinda não há avaliações
- Ozone Therapy by Saul Pressman at Oxygen Therapies Support Forum, Topic 443552 PDFDocumento15 páginasOzone Therapy by Saul Pressman at Oxygen Therapies Support Forum, Topic 443552 PDFHello MisterAinda não há avaliações
- Bio Project File 2Documento19 páginasBio Project File 2jiya singhAinda não há avaliações
- T1505C13Documento9 páginasT1505C13Gheorgian HageAinda não há avaliações
- Concept MapDocumento1 páginaConcept MapYalante BellAinda não há avaliações
- The Impact of Nurse Led Clinics On The Mortality.99638Documento7 páginasThe Impact of Nurse Led Clinics On The Mortality.99638Muhammad Badrushshalih100% (1)
- Fever in Children With ChemoteraphyDocumento23 páginasFever in Children With ChemoteraphyImanuel Far-FarAinda não há avaliações
- Case SheetDocumento23 páginasCase SheetMuhammad SdiqAinda não há avaliações
- Case ScenarioDocumento1 páginaCase ScenarioIrish Eunice FelixAinda não há avaliações
- SRH Case Study-GadDocumento7 páginasSRH Case Study-Gadapi-721737872Ainda não há avaliações
- Trade/Generic Name Classification Action of Medication Dosage/Route/ Frequency Indications For Use (Patient Specific)Documento16 páginasTrade/Generic Name Classification Action of Medication Dosage/Route/ Frequency Indications For Use (Patient Specific)lightzapAinda não há avaliações
- Use of Pallada in The Treatment of Allergic Conjunctivitis, Adenovirus Keratoconjunctivitis and KeratoconusDocumento4 páginasUse of Pallada in The Treatment of Allergic Conjunctivitis, Adenovirus Keratoconjunctivitis and KeratoconusCentral Asian StudiesAinda não há avaliações
- Transfusion Checklist Poster June 2021 Ver 1.0 1Documento1 páginaTransfusion Checklist Poster June 2021 Ver 1.0 1Naresh SinghAinda não há avaliações
- InhalantDocumento8 páginasInhalantArvin Ian Penaflor100% (1)
- Sephan Eve-In - Intensive - Care - Transport - VentilationDocumento4 páginasSephan Eve-In - Intensive - Care - Transport - VentilationzorgglubAinda não há avaliações
- Fundamental of Nursing-NleDocumento8 páginasFundamental of Nursing-NleJade DigoAinda não há avaliações
- UNCC300 Assesment TAsk 2Documento2 páginasUNCC300 Assesment TAsk 2Spandan DahalAinda não há avaliações
- 222Documento7 páginas222Erl DrizAinda não há avaliações
- P S Y C H O L O G I C Need Rest and Sleep Independent:: Nursing Care PlanDocumento1 páginaP S Y C H O L O G I C Need Rest and Sleep Independent:: Nursing Care Planunkown userAinda não há avaliações
- PDF Book UrduDocumento4 páginasPDF Book UrduMuhammad KamranAinda não há avaliações
- 1 Latifah Jehloh - งานนำเสนอDocumento41 páginas1 Latifah Jehloh - งานนำเสนอAisyahAinda não há avaliações