Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- HypoxiaDocumento21 páginasHypoxiaJojo RyelciusAinda não há avaliações
- Electronic Atlas of ParasitologyDocumento650 páginasElectronic Atlas of Parasitologystormyccs100% (7)
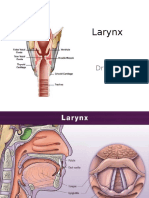
- LarynxDocumento34 páginasLarynxJojo Ryelcius100% (1)
- Abdominal WallDocumento75 páginasAbdominal WallJojo RyelciusAinda não há avaliações
- Struktur Clinical ReasoningDocumento15 páginasStruktur Clinical ReasoningJojo RyelciusAinda não há avaliações
- Stres Cairan Dan SuhuDocumento94 páginasStres Cairan Dan SuhuJojo RyelciusAinda não há avaliações
- Omega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenDocumento10 páginasOmega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenJojo RyelciusAinda não há avaliações
- FibrolipomaDocumento5 páginasFibrolipomaNarendra ChaudhariAinda não há avaliações
- Monday 7 January 2019: BiologyDocumento31 páginasMonday 7 January 2019: BiologyFathimathshaahaAinda não há avaliações
- Management of Renal Stones: Theme From January 2013 ExamDocumento123 páginasManagement of Renal Stones: Theme From January 2013 ExamBela VitoriaAinda não há avaliações
- Andrade, Ban, Salleva - Liver Cirrhosis - Objectives, Manifestations, Drug StudyDocumento9 páginasAndrade, Ban, Salleva - Liver Cirrhosis - Objectives, Manifestations, Drug StudyWindi Dawn SallevaAinda não há avaliações
- 13-05-2021 HMB EnglishDocumento82 páginas13-05-2021 HMB EnglishKiran SNAinda não há avaliações
- Simplified ACLS AlgorithmDocumento1 páginaSimplified ACLS AlgorithmBrianAinda não há avaliações
- 627-Texto Do Artigo-1922-1-10-20201125Documento5 páginas627-Texto Do Artigo-1922-1-10-20201125Daniel GuimarãesAinda não há avaliações
- Tahun Nomor NamaDocumento18 páginasTahun Nomor NamaALDO STEFANUZ (STIK)Ainda não há avaliações
- Future Growth PDFDocumento17 páginasFuture Growth PDFsaleem.aitmAinda não há avaliações
- Case Scenario 2 PDFDocumento7 páginasCase Scenario 2 PDFChristelle Ann FarralesAinda não há avaliações
- Ebook PDF Core Curriculum For Oncology Nursing 5th Edition PDFDocumento41 páginasEbook PDF Core Curriculum For Oncology Nursing 5th Edition PDFcarla.shurtliff473100% (40)
- Pengaruh Kompres Bawang Merah Terhadap Penurunan Suhu Tubuh Bayi Saat Demam Pasca Imunisasi Di Wilayah Kerja Polindes Pagar Ayu Musi RawasDocumento12 páginasPengaruh Kompres Bawang Merah Terhadap Penurunan Suhu Tubuh Bayi Saat Demam Pasca Imunisasi Di Wilayah Kerja Polindes Pagar Ayu Musi RawasAnisa SilviaAinda não há avaliações
- Induction and Augmentation of LaborDocumento20 páginasInduction and Augmentation of Laborjssamc prasootitantraAinda não há avaliações
- Rielle Bioethics AssDocumento7 páginasRielle Bioethics Assdrae syAinda não há avaliações
- Chapter 1 - Introduction and HistoryDocumento37 páginasChapter 1 - Introduction and HistoryTwinkle ParmarAinda não há avaliações
- CHN 4 RCDocumento11 páginasCHN 4 RCMarga AlvarezAinda não há avaliações
- AffiliationsDocumento9 páginasAffiliationsGurpreet CharaAinda não há avaliações
- List of Dissertation Topics RguhsDocumento5 páginasList of Dissertation Topics RguhsInstantPaperWriterSingapore100% (3)
- Current Research Areas - Psychology FacultyDocumento6 páginasCurrent Research Areas - Psychology FacultyAliya MojicaAinda não há avaliações
- Same-Day Sequential Cataract Surgery: Steve A. Arshinoff and Silvia OdorcicDocumento10 páginasSame-Day Sequential Cataract Surgery: Steve A. Arshinoff and Silvia OdorcicBenjamin NgAinda não há avaliações
- 3 Keys To Self Healing PDFDocumento10 páginas3 Keys To Self Healing PDFMircea MirceaAinda não há avaliações
- JFamCommunityMed262113-1349692 034456Documento5 páginasJFamCommunityMed262113-1349692 034456Putri Zatalini SabilaAinda não há avaliações
- Biomecanica Da ObesidadeDocumento9 páginasBiomecanica Da ObesidadehgtrainerAinda não há avaliações
- Z3rk4o00mfhmkk5mwrjowdDocumento2 páginasZ3rk4o00mfhmkk5mwrjowdVarun GognaAinda não há avaliações
- Disaster Preparation and Management For The Intensive Care UnitDocumento9 páginasDisaster Preparation and Management For The Intensive Care UnitSid DhayriAinda não há avaliações
- Assessment of Knowledge and Attitude of Pharmacists Toward The Side Effects of Anesthetics in Patients With Hypertension: A Cross-Sectional StudyDocumento9 páginasAssessment of Knowledge and Attitude of Pharmacists Toward The Side Effects of Anesthetics in Patients With Hypertension: A Cross-Sectional StudyMediterr J Pharm Pharm SciAinda não há avaliações
- NSCA Performance Training Journal (Conditioning May 2012)Documento27 páginasNSCA Performance Training Journal (Conditioning May 2012)Fitness Tutor for the ACE & NSCA Exams100% (4)
- Anemia: Clinical Approach and Management: Dairion Gatot, Savita Handayani, Heny Syahrini, Andri MardiaDocumento22 páginasAnemia: Clinical Approach and Management: Dairion Gatot, Savita Handayani, Heny Syahrini, Andri MardiarubyniAinda não há avaliações
- Welcome Aboard Crew Guide Book 11.02.00 - Rev. 44Documento17 páginasWelcome Aboard Crew Guide Book 11.02.00 - Rev. 44Click Technology100% (1)