Você também pode gostar
- Id 397 TeicoplaninDocumento2 páginasId 397 TeicoplaninStacey WoodsAinda não há avaliações
- Switching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilDocumento2 páginasSwitching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilGlory Claudia KarundengAinda não há avaliações
- IDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistDocumento3 páginasIDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistStacey WoodsAinda não há avaliações
- Critical CareDocumento8 páginasCritical CareDzikrul Haq KarimullahAinda não há avaliações
- Splenectomy Guideline Final 2012Documento6 páginasSplenectomy Guideline Final 2012Stacey WoodsAinda não há avaliações
- Management of Bacterial and Fungal Infections in Cirrhosis JOH 2021Documento17 páginasManagement of Bacterial and Fungal Infections in Cirrhosis JOH 2021Francisco Javier Gonzalez NomeAinda não há avaliações
- Palliative2 Nausea MedtableDocumento2 páginasPalliative2 Nausea MedtableStacey WoodsAinda não há avaliações
- Antithrombotic Therapy For VTE DiseaseDocumento13 páginasAntithrombotic Therapy For VTE DiseaseStacey WoodsAinda não há avaliações
- J Jacadv 2023 100389Documento12 páginasJ Jacadv 2023 100389Edward ElBuenoAinda não há avaliações
- 2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitDocumento19 páginas2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitStacey WoodsAinda não há avaliações
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocumento2 páginasTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsAinda não há avaliações
- Appropriate Use of Laxatives in The Older PersonDocumento7 páginasAppropriate Use of Laxatives in The Older PersonStacey WoodsAinda não há avaliações
- Potasio. 2014.Documento19 páginasPotasio. 2014.Nestor Enrique Aguilar SotoAinda não há avaliações
- Tamiflu PrescribingDocumento26 páginasTamiflu PrescribingStacey WoodsAinda não há avaliações
- Antibiotik WhoDocumento49 páginasAntibiotik WhodjebrutAinda não há avaliações
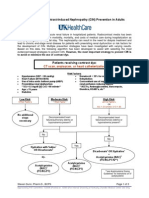
- Contrast NephRopathy GuidelinesDocumento3 páginasContrast NephRopathy GuidelinesStacey WoodsAinda não há avaliações
- Drug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseDocumento6 páginasDrug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseStacey WoodsAinda não há avaliações
- Antibiotic Selection - The Clinical AdvisorDocumento6 páginasAntibiotic Selection - The Clinical AdvisorStacey WoodsAinda não há avaliações
- StrokeDocumento2 páginasStrokeStacey WoodsAinda não há avaliações
- Procoagulant GuidelineDocumento30 páginasProcoagulant GuidelineStacey WoodsAinda não há avaliações
- C.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestDocumento2 páginasC.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestStacey WoodsAinda não há avaliações
- Antimicrobials at The End of LifeDocumento2 páginasAntimicrobials at The End of LifeStacey WoodsAinda não há avaliações
- Biomarkers of SepsisDocumento8 páginasBiomarkers of SepsisStacey WoodsAinda não há avaliações
- Fluid Choices Impact Outcome in Septic ShockDocumento7 páginasFluid Choices Impact Outcome in Septic ShockStacey WoodsAinda não há avaliações
- Stimulant May Speed Antidepressant Response Time in ElderlyDocumento3 páginasStimulant May Speed Antidepressant Response Time in ElderlyStacey WoodsAinda não há avaliações
- Elderly Patients Making Wise ChoicesDocumento6 páginasElderly Patients Making Wise ChoicesStacey WoodsAinda não há avaliações
- Preoperative Insulin 2013Documento3 páginasPreoperative Insulin 2013Stacey WoodsAinda não há avaliações
- Airway Clearance in The Intensive Care UnitDocumento5 páginasAirway Clearance in The Intensive Care UnitStacey WoodsAinda não há avaliações
- The ABC of Weaning Failure - A Structured ApproachDocumento9 páginasThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- IDR 69596 Profile of Efinaconazole in The Treatment of Onchomycosis 060115Documento10 páginasIDR 69596 Profile of Efinaconazole in The Treatment of Onchomycosis 060115intankmlsAinda não há avaliações
- ICH Public Meeting Amsterdam 042919Documento125 páginasICH Public Meeting Amsterdam 042919Jose De La Cruz De La O100% (1)
- Non Surgical Fat ReductionDocumento12 páginasNon Surgical Fat ReductionadeAinda não há avaliações
- Kanchana Allan Nursing Resume - New Grad PositionDocumento3 páginasKanchana Allan Nursing Resume - New Grad Positionapi-416448549Ainda não há avaliações
- Fundamentials of Shared Service OperationsDocumento125 páginasFundamentials of Shared Service OperationsОлег Дрошнев100% (3)
- Hiv/aids JournalDocumento9 páginasHiv/aids JournalStar AlvarezAinda não há avaliações
- GSK Case Study & PR PlanDocumento475 páginasGSK Case Study & PR PlanJBull7645100% (1)
- 2010-2011 Annual ReportDocumento130 páginas2010-2011 Annual ReportSlusom WebAinda não há avaliações
- 21cfr11 Checklist (CFR)Documento2 páginas21cfr11 Checklist (CFR)marco_fmAinda não há avaliações
- 108-Epidemiological Studies - A Practical Guide, 2nd Edition-Alan J. Silman Gary J. Macfarlane-05 PDFDocumento256 páginas108-Epidemiological Studies - A Practical Guide, 2nd Edition-Alan J. Silman Gary J. Macfarlane-05 PDFMarisela Fuentes100% (1)
- Acceptability: ©WHO/Sergey VolkovDocumento26 páginasAcceptability: ©WHO/Sergey VolkovBeatriz PatricioAinda não há avaliações
- Adverse Event TemplateDocumento5 páginasAdverse Event TemplateGocThuGianAinda não há avaliações
- Ivermectin For Prophylaxis and Treatment of Covid 19Documento2 páginasIvermectin For Prophylaxis and Treatment of Covid 19jermAinda não há avaliações
- Revised Guidelines on Surveillance and Response to Adverse Events Following ImmunizationDocumento22 páginasRevised Guidelines on Surveillance and Response to Adverse Events Following ImmunizationReanne Pauline Manipon100% (2)
- Reseach (Case Study)Documento25 páginasReseach (Case Study)salahnaser9999Ainda não há avaliações
- MicroCap Review Spring 2019Documento96 páginasMicroCap Review Spring 2019Planet MicroCap Review Magazine67% (3)
- Institute of Lung Health Leicester: Shane CariasDocumento10 páginasInstitute of Lung Health Leicester: Shane CariasShane CariasAinda não há avaliações
- Improving Methods For Estimating Cost of Production in Developing Countries Report JRC Lit Review PDFDocumento19 páginasImproving Methods For Estimating Cost of Production in Developing Countries Report JRC Lit Review PDFHarshithaAinda não há avaliações
- Computers in Biology and MedicineDocumento16 páginasComputers in Biology and MedicineDhanalekshmi YedurkarAinda não há avaliações
- 6 April 2023 Academic Reading Practice TestDocumento14 páginas6 April 2023 Academic Reading Practice TestNguyễn Chính ThạoAinda não há avaliações
- Vaccinepeerreview PDFDocumento1.053 páginasVaccinepeerreview PDFMatthew SharpAinda não há avaliações
- New Drug Application Nda ChecklistDocumento6 páginasNew Drug Application Nda Checklistjzames001Ainda não há avaliações
- Part 1: Introduction Part 2: Responsibilities by Role Part 3: Summary of Key PointsDocumento13 páginasPart 1: Introduction Part 2: Responsibilities by Role Part 3: Summary of Key PointsFaye BaliloAinda não há avaliações
- Submissions & Author Guidelines - American Dental Association - ADADocumento8 páginasSubmissions & Author Guidelines - American Dental Association - ADAjennys420Ainda não há avaliações
- Icoffee Journal 2k22Documento5 páginasIcoffee Journal 2k22Ayur Manthra OrgAinda não há avaliações
- C0EF-1BE9 Dental Medical 4 5825818559418206088 PDFDocumento130 páginasC0EF-1BE9 Dental Medical 4 5825818559418206088 PDFOctavian CiceuAinda não há avaliações
- Pharm NotesDocumento198 páginasPharm NotesNancy Danielz80% (5)
- Boost Community Understanding of Youth LibraryDocumento30 páginasBoost Community Understanding of Youth LibraryErgado A. Aman86% (7)
- Ich-Guideline-S10-Photosafety-Evaluation-Pharmaceuticals-Step-5 - enDocumento17 páginasIch-Guideline-S10-Photosafety-Evaluation-Pharmaceuticals-Step-5 - enHasna Ulya AnnafisAinda não há avaliações
- EUROPEAN COMMISSION CLINICAL TRIALS GUIDANCEDocumento56 páginasEUROPEAN COMMISSION CLINICAL TRIALS GUIDANCEgwapingMDAinda não há avaliações