Você também pode gostar
- Operations Management Rock Salt ResultsDocumento3 páginasOperations Management Rock Salt ResultsEdwin MasirorAinda não há avaliações
- SNPG918 Critical Appraisal Marking Guide Assessment 2Documento1 páginaSNPG918 Critical Appraisal Marking Guide Assessment 2Edwin MasirorAinda não há avaliações
- Australia Waste ManagementDocumento2 páginasAustralia Waste ManagementEdwin MasirorAinda não há avaliações
- Current Issues in Contemporary People ManagementDocumento8 páginasCurrent Issues in Contemporary People ManagementEdwin MasirorAinda não há avaliações
- Launching Kmart in IndiaDocumento15 páginasLaunching Kmart in IndiaEdwin MasirorAinda não há avaliações
- Sustainable Warehouse ManagementDocumento8 páginasSustainable Warehouse ManagementEdwin Masiror100% (1)
- Sustainable Warehouse ManagementDocumento8 páginasSustainable Warehouse ManagementEdwin Masiror100% (1)
- Reflective Report Inventory BasicsDocumento3 páginasReflective Report Inventory BasicsEdwin Masiror100% (5)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Ferrography/oil Analysis: An Excellent Condition Monitoring TechniqueDocumento5 páginasFerrography/oil Analysis: An Excellent Condition Monitoring Techniquedaniel zorroAinda não há avaliações
- The Information Age CHAPTER 7 StsDocumento7 páginasThe Information Age CHAPTER 7 StsAngel FlordelizaAinda não há avaliações
- Introduction To Stainless SteelDocumento19 páginasIntroduction To Stainless Steelkrishna chiruAinda não há avaliações
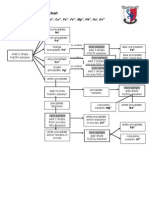
- Testing For Cations Flow ChartDocumento2 páginasTesting For Cations Flow Chartapi-252561013Ainda não há avaliações
- Kmartinez Draft Research PaperDocumento14 páginasKmartinez Draft Research Paperapi-273007806Ainda não há avaliações
- Exp 4 Centrifugal CompressorDocumento11 páginasExp 4 Centrifugal CompressorFaris HamirAinda não há avaliações
- RBC Disorder BcqsDocumento68 páginasRBC Disorder BcqsMukhtiar AhmedAinda não há avaliações
- Juri Ferrer - Ws - WeatherDocumento4 páginasJuri Ferrer - Ws - WeathersJIqsAinda não há avaliações
- Summary (Adjuncts)Documento2 páginasSummary (Adjuncts)Ngọc MinhAinda não há avaliações
- 6 Human Diseases That Cause by VirusesDocumento7 páginas6 Human Diseases That Cause by VirusesJefry JapAinda não há avaliações
- Tibia Bone Segmentation in X-Ray Images - A Comparative AnalysisDocumento8 páginasTibia Bone Segmentation in X-Ray Images - A Comparative AnalysisSuzanaPetrovicAinda não há avaliações
- Leonard Peikoff-Introduction To LogicDocumento20 páginasLeonard Peikoff-Introduction To Logicbursa07Ainda não há avaliações
- Midterm2 KeyDocumento6 páginasMidterm2 KeyHungDoAinda não há avaliações
- Psicologia BuenisimoDocumento6 páginasPsicologia BuenisimoSophieAinda não há avaliações
- AssaultDocumento12 páginasAssaultEd Mundo100% (3)
- Bycatch Reduction Devices - PresentationDocumento92 páginasBycatch Reduction Devices - PresentationSujit Shandilya0% (1)
- POFL Unit 1 Status QUO pp.1-37Documento38 páginasPOFL Unit 1 Status QUO pp.1-37AruAinda não há avaliações
- LabStan - July 16-17, 23-24, 30-31, Aug 6-7Documento25 páginasLabStan - July 16-17, 23-24, 30-31, Aug 6-7CandypopAinda não há avaliações
- Sensus 143-80 Service Regulator R-1301 R5Documento11 páginasSensus 143-80 Service Regulator R-1301 R5Paolita Auza BalderramaAinda não há avaliações
- Lead in Water: Standard Test Methods ForDocumento17 páginasLead in Water: Standard Test Methods ForAMMARAinda não há avaliações
- CAST Optical Smoke Detector: Part NoDocumento3 páginasCAST Optical Smoke Detector: Part NoAnis TantoushAinda não há avaliações
- Diana ACCOMPLISHMENTDocumento8 páginasDiana ACCOMPLISHMENTMarycon MaapoyAinda não há avaliações
- World Wide Emission Free E-Motercycle ProjectDocumento20 páginasWorld Wide Emission Free E-Motercycle ProjectAkshay SharmaAinda não há avaliações
- MSW TACSOP v.3.3Documento59 páginasMSW TACSOP v.3.3Mira BellaAinda não há avaliações
- CS1 Epoxy Curing AgentsDocumento21 páginasCS1 Epoxy Curing AgentsAlptekin100% (1)
- Fitting in and Fighting Back: Stigma Management Strategies Among Homeless KidsDocumento24 páginasFitting in and Fighting Back: Stigma Management Strategies Among Homeless KidsIrisha AnandAinda não há avaliações
- Grade 10 Chemistry Week 1Documento3 páginasGrade 10 Chemistry Week 1Nikoli MajorAinda não há avaliações
- Manual Servicio Soxte 2050Documento46 páginasManual Servicio Soxte 2050Quimica JordanlabAinda não há avaliações
- The Bitter Internal Drive of AppleDocumento7 páginasThe Bitter Internal Drive of AppleBon WambuaAinda não há avaliações
- Herbs and SpicesDocumento77 páginasHerbs and SpicesNicole RicohermosoAinda não há avaliações