Você também pode gostar
- Dragon's Touch (Exerpt) - Hei Long - Paladin Press PDFDocumento6 páginasDragon's Touch (Exerpt) - Hei Long - Paladin Press PDFbizasephiroth100% (2)
- General Exam and Q&A For MBBS DR ShamolDocumento320 páginasGeneral Exam and Q&A For MBBS DR Shamolmaybe100% (3)
- Abnormal EcgDocumento8 páginasAbnormal EcgM.DalaniAinda não há avaliações
- ABC of Reading Chest XrayDocumento1 páginaABC of Reading Chest Xraykrisnochura100% (3)
- CardiologyDocumento6 páginasCardiologyFrancis FransAinda não há avaliações
- Abdominal Examination - OSCE Guide - Geeky MedicsDocumento9 páginasAbdominal Examination - OSCE Guide - Geeky MedicsJahangir Alam100% (1)
- Cardiovascular ExaminationDocumento13 páginasCardiovascular ExaminationBitu JaaAinda não há avaliações
- Chest X-RayDocumento125 páginasChest X-RayRusda Syawie100% (1)
- Chest X RayDocumento61 páginasChest X RayP Vinod Kumar100% (1)
- Clinical Exam NotesDocumento222 páginasClinical Exam Notesakansha_bhargava_6100% (1)
- Clinical ExaminationDocumento11 páginasClinical ExaminationMavra zAinda não há avaliações
- Chest X-Ray Interpretation A Structured Approach Radiology OSCEDocumento1 páginaChest X-Ray Interpretation A Structured Approach Radiology OSCEValentina SepúlvedaAinda não há avaliações
- 5th Year General Surgery Notes - Lower GIT SurgeryDocumento3 páginas5th Year General Surgery Notes - Lower GIT SurgeryJason HarryAinda não há avaliações
- Bones PDFDocumento227 páginasBones PDFAtthapu ThirupathaiahAinda não há avaliações
- Chest X Ray Diagnostic AlgorithmDocumento10 páginasChest X Ray Diagnostic AlgorithmCalin Popa100% (1)
- Cardiovascular ExaminationDocumento5 páginasCardiovascular ExaminationMTBRISCOEAinda não há avaliações
- The Girdles Sternum and Paired AppendagesDocumento9 páginasThe Girdles Sternum and Paired AppendagesAmberValentineAinda não há avaliações
- BonesDocumento2 páginasBonesEsther Prieto ChinéAinda não há avaliações
- Nov AIIMS 2018 Pathology Questions and Explanations by Dr. SUSHANT SONIDocumento9 páginasNov AIIMS 2018 Pathology Questions and Explanations by Dr. SUSHANT SONIZahidha BegumAinda não há avaliações
- Mobilization NotesDocumento239 páginasMobilization NotesSuganya Balachandran100% (6)
- Chest X Ray Made SimpleDocumento103 páginasChest X Ray Made SimpleMayer Rosenberg100% (18)
- History and Causology - DR - ShamolDocumento265 páginasHistory and Causology - DR - ShamolUmer Farooq100% (1)
- Cardiovascular Examination GuideDocumento2 páginasCardiovascular Examination Guiderhea100% (1)
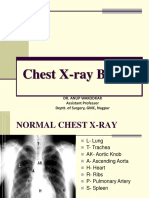
- Chest X Ray BasicsDocumento99 páginasChest X Ray BasicsHarshaWakodkarAinda não há avaliações
- Chest X-Ray InterpretationDocumento14 páginasChest X-Ray InterpretationKoya AnushareddyAinda não há avaliações
- Cardiovascular Examination Checklist OSCEDocumento1 páginaCardiovascular Examination Checklist OSCESteve TanAinda não há avaliações
- CHEST X-RAY Presentation CVSDocumento45 páginasCHEST X-RAY Presentation CVSNorsafrini Rita Ahmad100% (1)
- Thyroid Case ProformaDocumento2 páginasThyroid Case ProformaSneha NaulakhaAinda não há avaliações
- Skeletal System PowerPointDocumento37 páginasSkeletal System PowerPointScience,Physical Education And Sports Videos100% (1)
- RX Protocol by DR - Anwarul Azim PDFDocumento120 páginasRX Protocol by DR - Anwarul Azim PDFGB Majumder100% (1)
- DIFFERENTIALS and MnemonicsDocumento20 páginasDIFFERENTIALS and MnemonicsqurbanAinda não há avaliações
- Abdominal Xray Interpretation and Cases For FinalsDocumento39 páginasAbdominal Xray Interpretation and Cases For Finalsfahadrock2002Ainda não há avaliações
- RX ProtocolDocumento120 páginasRX ProtocolIAMSANWAR019170100% (5)
- GIT OSCE (Week 9) : Mention You Would Observe General Appearance and Take VitalsDocumento3 páginasGIT OSCE (Week 9) : Mention You Would Observe General Appearance and Take Vitalsrenae_vardAinda não há avaliações
- Ultrasound Made EasyDocumento7 páginasUltrasound Made EasyAnonymous ZUaUz1wwAinda não há avaliações
- 008 Plain X-Ray AbdomenDocumento7 páginas008 Plain X-Ray AbdomenAthul GurudasAinda não há avaliações
- Right Hypochondrium2Documento4 páginasRight Hypochondrium2Subash KarkiAinda não há avaliações
- Problem-based Approach to Gastroenterology and HepatologyNo EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAinda não há avaliações
- OSCE-Surgery Block PDFDocumento31 páginasOSCE-Surgery Block PDFmisstina.19876007100% (2)
- Ultrasound Measurement Cheat SheetDocumento1 páginaUltrasound Measurement Cheat SheetDr. MLKAinda não há avaliações
- CLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSNo EverandCLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSAinda não há avaliações
- Almaghrabi Abdomen ExaminationDocumento27 páginasAlmaghrabi Abdomen ExaminationSagit Nauman81100% (1)
- Macrocosmic OrbitDocumento14 páginasMacrocosmic OrbitRudy100% (1)
- Abdo and HerniasDocumento6 páginasAbdo and Herniasjoedeegan_Ainda não há avaliações
- PVD Case ProformaDocumento2 páginasPVD Case ProformaRiyaSinghAinda não há avaliações
- ECG DR ShamolDocumento574 páginasECG DR ShamolSajib Nakib91% (11)
- Thyroid Examination FiryaLDocumento3 páginasThyroid Examination FiryaLFiryal Balushi100% (1)
- Skeletal System PowerpointDocumento40 páginasSkeletal System PowerpointMugabi Fahad100% (1)
- 7.saq Miscellaneous QuestionsDocumento554 páginas7.saq Miscellaneous QuestionsdoctorirfanAinda não há avaliações
- Surgery Viva QuestionsDocumento16 páginasSurgery Viva QuestionsChris Lam Cui ShanAinda não há avaliações
- I. Inspection: Cardiovascular ExamDocumento136 páginasI. Inspection: Cardiovascular ExamMarbella39Ainda não há avaliações
- Clavicle Plate and Screw System Surgical TechniqueDocumento12 páginasClavicle Plate and Screw System Surgical TechniqueDrvijay Saradhara100% (1)
- Respiratory Assessment 2Documento24 páginasRespiratory Assessment 2Kendal BartonAinda não há avaliações
- Thyroid CaseDocumento53 páginasThyroid CaseKenisha HutsonAinda não há avaliações
- HyphemaDocumento19 páginasHyphemaLiyanti RinceAinda não há avaliações
- History SummaryDocumento233 páginasHistory SummarymaybeAinda não há avaliações
- Cardiology OSCEDocumento35 páginasCardiology OSCEvigneshmmc02Ainda não há avaliações
- Pre Exam Surgical Notes 2Documento166 páginasPre Exam Surgical Notes 2flor vickyAinda não há avaliações
- Cardiovascular BigDocumento37 páginasCardiovascular Bigfaiz nasirAinda não há avaliações
- Surg Osce SummaryDocumento7 páginasSurg Osce SummaryShatha AlgahtaniAinda não há avaliações
- Shivaani (Internal Medicine CWU)Documento12 páginasShivaani (Internal Medicine CWU)S.M. Manogaran Shivaani AP S.M. ManogaranAinda não há avaliações
- Acute Abdominal Pain History and Exam HPCDocumento5 páginasAcute Abdominal Pain History and Exam HPCnaafAinda não há avaliações
- OSCE Internal MedicineDocumento4 páginasOSCE Internal Medicinemohamed mowafeyAinda não há avaliações
- Mitral Stenosis, NicvdDocumento33 páginasMitral Stenosis, NicvdNavojit ChowdhuryAinda não há avaliações
- Valvular Heart Disease 2Documento46 páginasValvular Heart Disease 2Topea BogdanAinda não há avaliações
- CXR Interpretation WriteupDocumento32 páginasCXR Interpretation WriteupArhanAinda não há avaliações
- COVID - English Final PDFDocumento2 páginasCOVID - English Final PDFazar103Ainda não há avaliações
- TNSOP 2 Sample Collection PDFDocumento4 páginasTNSOP 2 Sample Collection PDFazar103Ainda não há avaliações
- TNSOP 6 Clinical GuidelinesDocumento14 páginasTNSOP 6 Clinical Guidelinesazar103Ainda não há avaliações
- TNSOP 4 Home Care PDFDocumento1 páginaTNSOP 4 Home Care PDFazar103Ainda não há avaliações
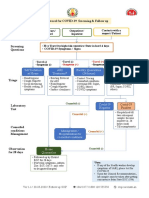
- Protocol For COVID 19 Screening and Followup PDFDocumento1 páginaProtocol For COVID 19 Screening and Followup PDFazar103Ainda não há avaliações
- Contact Follow Up: Identify Contacts of Lab Confirmed COVID-19 Patients by District EOC (Use FORM 3A)Documento1 páginaContact Follow Up: Identify Contacts of Lab Confirmed COVID-19 Patients by District EOC (Use FORM 3A)azar103Ainda não há avaliações
- The Shoulder GirdleDocumento26 páginasThe Shoulder GirdleVeena VishwanathAinda não há avaliações
- Autopsy Report For Jonathan FerrellDocumento11 páginasAutopsy Report For Jonathan FerrellWFAE 90.7 FMAinda não há avaliações
- Jinlei Li, Wei Jiang, Nalini Vadivelu - First Aid Perioperative Ultrasound - Acute Pain Manual For Surgical Procedures (2023, Springer)Documento668 páginasJinlei Li, Wei Jiang, Nalini Vadivelu - First Aid Perioperative Ultrasound - Acute Pain Manual For Surgical Procedures (2023, Springer)Inês BatistaAinda não há avaliações
- The Coaches Guide To Bicipital Tendonitis PDFDocumento8 páginasThe Coaches Guide To Bicipital Tendonitis PDFYuldashAinda não há avaliações
- Oatis - CH08 117 149 PDFDocumento33 páginasOatis - CH08 117 149 PDFKanwal KhanAinda não há avaliações
- Osteology BonesDocumento48 páginasOsteology BonesÂhmęd ĐoolaAinda não há avaliações
- Fundamentals of Anatomy and Physiology 10th Edition Martini Solutions Manual 1Documento36 páginasFundamentals of Anatomy and Physiology 10th Edition Martini Solutions Manual 1toddvaldezamzxfwnrtq97% (29)
- Scan 13 Sep 2019Documento25 páginasScan 13 Sep 2019Deepak ChauhanAinda não há avaliações
- 1-Bones of The Upper Limb Final-2Documento18 páginas1-Bones of The Upper Limb Final-2DrVasu Mudiraj100% (1)
- Ortho Services Sports Rehab Clavicle Fracture Protocol Non SurgicalDocumento17 páginasOrtho Services Sports Rehab Clavicle Fracture Protocol Non SurgicalKattamedhi Krishnachaitanya KumarreddyAinda não há avaliações
- The Anatomy of Medical Terminology Chapter 3Documento7 páginasThe Anatomy of Medical Terminology Chapter 3Gregg ProducerAinda não há avaliações
- 1 Osteology (MCQ)Documento12 páginas1 Osteology (MCQ)Utkarsh MishraAinda não há avaliações
- 2002, Vol.33, Issues 1, Treatment of Complex FracturesDocumento280 páginas2002, Vol.33, Issues 1, Treatment of Complex FracturesSitthikorn StrikerrAinda não há avaliações
- Ayomisola MCQDocumento15 páginasAyomisola MCQTeeAinda não há avaliações
- Acland Human AnatomyDocumento51 páginasAcland Human Anatomyjust for download matterAinda não há avaliações
- 1 ANT Anatomy of The Upper Limp TGDocumento129 páginas1 ANT Anatomy of The Upper Limp TGReath Gatkuoth DuothAinda não há avaliações
- The Skeleton: Chapter 7 Part CDocumento73 páginasThe Skeleton: Chapter 7 Part CDon KeyAinda não há avaliações
- Anatomi Dan Kinesiologi Shoulder Part 2Documento38 páginasAnatomi Dan Kinesiologi Shoulder Part 2denishAinda não há avaliações
- Modifications of Appendicular Skeletons in VertebrateDocumento25 páginasModifications of Appendicular Skeletons in Vertebratekhansalma3399Ainda não há avaliações
- Skeletal System Reading Comprehension Exercises - 126764Documento5 páginasSkeletal System Reading Comprehension Exercises - 126764Lucianny FilionAinda não há avaliações
- OsteologyDocumento96 páginasOsteologyBenita Putri MD100% (2)