Você também pode gostar
- ESBL Phenotipic PDFDocumento14 páginasESBL Phenotipic PDFGerardo J. Huerta RoblesAinda não há avaliações
- Praktikum Mikrobiologi Gram NegatifDocumento44 páginasPraktikum Mikrobiologi Gram Negatifrids_Ainda não há avaliações
- HCL Update 2019 PDFDocumento8 páginasHCL Update 2019 PDFHaroon KhanAinda não há avaliações
- Lecture 27-Basic Virology-Dr. Ludhang Pradipta Rizki, M.biotech, SP - MK (2018)Documento45 páginasLecture 27-Basic Virology-Dr. Ludhang Pradipta Rizki, M.biotech, SP - MK (2018)NOVI UMAMI UMAMIAinda não há avaliações
- Respon Imun Terhadap PenyakitDocumento40 páginasRespon Imun Terhadap PenyakitKolor GantengAinda não há avaliações
- Immunity To MicrobesDocumento25 páginasImmunity To MicrobestimcarasAinda não há avaliações
- EsblDocumento16 páginasEsblsharmamaddy32Ainda não há avaliações
- 2-Microscopic IdentificationDocumento24 páginas2-Microscopic IdentificationMunir AhmedAinda não há avaliações
- Pengaruh Intensitas Cahaya Dan Nutrisi Terhadap Pertumbuhan MiseliumDocumento6 páginasPengaruh Intensitas Cahaya Dan Nutrisi Terhadap Pertumbuhan MiseliumPUTRI ZAKY ALVAS SYAHNIARAinda não há avaliações
- Tes Lab Pada Peny Infeksi Dan Tropis (Lebih Singkat)Documento71 páginasTes Lab Pada Peny Infeksi Dan Tropis (Lebih Singkat)Monazzt AsshagabAinda não há avaliações
- EsblDocumento159 páginasEsblArunagiri Subramanian100% (2)
- Multiple Myeloma OverviewDocumento52 páginasMultiple Myeloma OverviewanmegpraAinda não há avaliações
- AFPDocumento4 páginasAFPHassan GillAinda não há avaliações
- What'S New in Treatment Monitoring: Viral Load and Cd4 TestingDocumento2 páginasWhat'S New in Treatment Monitoring: Viral Load and Cd4 TestingRina ErlinaAinda não há avaliações
- Quorum Sensing in Bacteria and A Glance On Pseudomonas Aeruginosa 2327 5073.1000156Documento10 páginasQuorum Sensing in Bacteria and A Glance On Pseudomonas Aeruginosa 2327 5073.1000156Tanjila IslamAinda não há avaliações
- MULTIPLE MYELOMA For Medical Students. Copy - 032148Documento39 páginasMULTIPLE MYELOMA For Medical Students. Copy - 032148Miracle Odenigbo100% (1)
- Para Protein Emi ADocumento14 páginasPara Protein Emi AMohamoud MohamedAinda não há avaliações
- Virology Techniques: Chapter 5 - Lesson 4Documento8 páginasVirology Techniques: Chapter 5 - Lesson 4Ramling PatrakarAinda não há avaliações
- Carbapenem Resistance A ReviewDocumento28 páginasCarbapenem Resistance A ReviewSri IriantiAinda não há avaliações
- Anti-Mutated Citrullinated Vimentin Antibodies in Rheumatoid ArthritisDocumento17 páginasAnti-Mutated Citrullinated Vimentin Antibodies in Rheumatoid ArthritisReda RamzyAinda não há avaliações
- Blind PassagingDocumento1 páginaBlind PassagingsomchaisAinda não há avaliações
- Lab Report 10Documento6 páginasLab Report 10api-301352285Ainda não há avaliações
- Final Announcement MaGEHUp 2022Documento14 páginasFinal Announcement MaGEHUp 2022Teti HendrayaniAinda não há avaliações
- ID Virus Avian Influenza h5n1 Biologi Molek PDFDocumento13 páginasID Virus Avian Influenza h5n1 Biologi Molek PDFArsienda UlmafemaAinda não há avaliações
- Lowenstein Jensen MediumDocumento2 páginasLowenstein Jensen MediumRizal IchwansyahAinda não há avaliações
- Hematology 2Documento58 páginasHematology 2Laboratorium Ansari SalehAinda não há avaliações
- Multiple MyelomaDocumento15 páginasMultiple MyelomaDinda YusditiraAinda não há avaliações
- Oncogenesis Topic by Laraib FiazDocumento23 páginasOncogenesis Topic by Laraib FiazLaraib FiazAinda não há avaliações
- Ca 125Documento3 páginasCa 125डा. सत्यदेव त्यागी आर्यAinda não há avaliações
- 15) Dr. Firdaus, Ph. D - Penjelasan Praktikum REPRODUKSI PALUDocumento35 páginas15) Dr. Firdaus, Ph. D - Penjelasan Praktikum REPRODUKSI PALUcimyAinda não há avaliações
- Acinetobacter Baumannii by Gemechis DejeneDocumento36 páginasAcinetobacter Baumannii by Gemechis DejeneGemechis DejeneAinda não há avaliações
- Alpha FetoproteinDocumento2 páginasAlpha FetoproteinmonimoyAinda não há avaliações
- 1 Introduction SymbiosisDocumento229 páginas1 Introduction Symbiosisbex9gg100% (1)
- Immunofluorescence: Tapeshwar Yadav (Lecturer)Documento23 páginasImmunofluorescence: Tapeshwar Yadav (Lecturer)Raj Kumar SoniAinda não há avaliações
- TB Meningitis Lancet 2022Documento15 páginasTB Meningitis Lancet 2022stephanie bojorquezAinda não há avaliações
- Microcytic Anemia PDFDocumento8 páginasMicrocytic Anemia PDFMargarita TorresAinda não há avaliações
- Gene Expression: Protein Synthesis and Control RNA Synthesis and Control Chromatin Structure and FunctionNo EverandGene Expression: Protein Synthesis and Control RNA Synthesis and Control Chromatin Structure and FunctionBrian F. C. ClarkAinda não há avaliações
- Carbapenamases Facts and DetecctionDocumento68 páginasCarbapenamases Facts and Detecctiontummalapalli venkateswara raoAinda não há avaliações
- Review Article - Mirizzi SyndromeDocumento4 páginasReview Article - Mirizzi SyndromeEvan KristionoAinda não há avaliações
- Comparison TB LAMP, Microscopy, GeneXpert and CultureDocumento24 páginasComparison TB LAMP, Microscopy, GeneXpert and Culturepolosan123Ainda não há avaliações
- FACSDocumento24 páginasFACSMudit MisraAinda não há avaliações
- Pratiwi S Gunawan, BDS., DDS., MDSC, PHDDocumento53 páginasPratiwi S Gunawan, BDS., DDS., MDSC, PHDBima Ewando KabanAinda não há avaliações
- HEMATOPOIESISDocumento44 páginasHEMATOPOIESISviviyanti znAinda não há avaliações
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocumento18 páginasMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaAinda não há avaliações
- 1.1 Bacterial Morphology Structure and ClassificationDocumento108 páginas1.1 Bacterial Morphology Structure and ClassificationJustine Mel Concepcion IlardeAinda não há avaliações
- Principle of VaccineDocumento10 páginasPrinciple of VaccineRasyid WicaksonoAinda não há avaliações
- Alpha Fetoprotein (Afp)Documento10 páginasAlpha Fetoprotein (Afp)Andi UkengAinda não há avaliações
- Carbapenem Power PointDocumento34 páginasCarbapenem Power PointAbiola Olumuyiwa OlaitanAinda não há avaliações
- New Red Blood Cell and Reticulocyte Parameters and Reference Values For Healthy Individuals and in Chronic Kidney Disease.Documento8 páginasNew Red Blood Cell and Reticulocyte Parameters and Reference Values For Healthy Individuals and in Chronic Kidney Disease.Alberto MarcosAinda não há avaliações
- Tumor Markeri - Eng PDFDocumento79 páginasTumor Markeri - Eng PDFdr_4uAinda não há avaliações
- Pancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseDocumento6 páginasPancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseIJAR JOURNALAinda não há avaliações
- BCCA Febrile Neutropenia GuidelinesDocumento2 páginasBCCA Febrile Neutropenia GuidelinesdenokayuMRAinda não há avaliações
- CBA MouseTh1Th2 Kit ManualDocumento52 páginasCBA MouseTh1Th2 Kit ManualendopetAinda não há avaliações
- Jurnal RubellaDocumento2 páginasJurnal RubellaAlif SpiritAinda não há avaliações
- Cystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 DiabetesDocumento9 páginasCystatin C As An Early Marker of Diabetic Nephropathy in Nigerian Adults With Type 2 Diabetesijmb333Ainda não há avaliações
- "Simple Screening Test of Ampc Beta-Lactamases in Clinical Isolates Among MultidrugDocumento15 páginas"Simple Screening Test of Ampc Beta-Lactamases in Clinical Isolates Among MultidrugBhagwat Suryawanshi100% (1)
- Tuberculosis en PDFDocumento307 páginasTuberculosis en PDFAbdullah Khairul AfnanAinda não há avaliações
- Acute-On-Chronic Liver Failure - Controversies and ConsensusDocumento10 páginasAcute-On-Chronic Liver Failure - Controversies and ConsensusPhan Nguyễn Đại NghĩaAinda não há avaliações
- Jurnal Gastroenterology, Hepatology, and Nutrition PediatricDocumento71 páginasJurnal Gastroenterology, Hepatology, and Nutrition PediatricJonathan WelchAinda não há avaliações
- Pediatric Neurology PDFDocumento301 páginasPediatric Neurology PDFJonathan WelchAinda não há avaliações
- Pediatric Gastroenterology Algorithme PDFDocumento118 páginasPediatric Gastroenterology Algorithme PDFJonathan Welch100% (1)
- TB SimulationDocumento15 páginasTB SimulationJonathan WelchAinda não há avaliações
- International Journal of Pathology and Clinical Research Ijpcr 2 023Documento9 páginasInternational Journal of Pathology and Clinical Research Ijpcr 2 023Jonathan WelchAinda não há avaliações
- Glasgow Meningococcal Septicaemia Prognostic Score (GMPS) : Arrival 1 Hour 1 Systolic Blood PressureDocumento1 páginaGlasgow Meningococcal Septicaemia Prognostic Score (GMPS) : Arrival 1 Hour 1 Systolic Blood PressureJonathan WelchAinda não há avaliações
- Antibiotik Pada Anak: Achmad Yudha ApDocumento23 páginasAntibiotik Pada Anak: Achmad Yudha ApJonathan WelchAinda não há avaliações
- Clinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants PDFDocumento27 páginasClinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants PDFJonathan WelchAinda não há avaliações
- Causedoutbreak Klebsiella PDFDocumento11 páginasCausedoutbreak Klebsiella PDFJonathan WelchAinda não há avaliações
- Ta Katsuji 1996Documento7 páginasTa Katsuji 1996Jonathan WelchAinda não há avaliações
- Laura M Lamberti, Christa L Fischer Walker, Adi Noiman, Cesar Victora and Robert E BlackDocumento1 páginaLaura M Lamberti, Christa L Fischer Walker, Adi Noiman, Cesar Victora and Robert E BlackJonathan WelchAinda não há avaliações
- Esbl Sepsis India2011Documento8 páginasEsbl Sepsis India2011Jonathan WelchAinda não há avaliações
- Early-Onset Neonatal Sepsis: Kari A. Simonsen, Ann L. Anderson-Berry, Shirley F. Delair, H. Dele DaviesDocumento27 páginasEarly-Onset Neonatal Sepsis: Kari A. Simonsen, Ann L. Anderson-Berry, Shirley F. Delair, H. Dele DaviesJonathan WelchAinda não há avaliações
- MGMTDocumento19 páginasMGMTMakrant MohanAinda não há avaliações
- A656 GR 80 Brochure 06-26-08Documento2 páginasA656 GR 80 Brochure 06-26-08OsmanAinda não há avaliações
- Soft Tissue SarcomaDocumento19 páginasSoft Tissue SarcomaEkvanDanangAinda não há avaliações
- BT HandoutsDocumento4 páginasBT HandoutsNerinel CoronadoAinda não há avaliações
- OBESITY - Cayce Health DatabaseDocumento4 páginasOBESITY - Cayce Health Databasewcwjr55Ainda não há avaliações
- Speaking Topics For Final ReviewDocumento3 páginasSpeaking Topics For Final ReviewNhư ÝAinda não há avaliações
- BDC 6566Documento6 páginasBDC 6566jack.simpson.changAinda não há avaliações
- HDFC Life Insurance (HDFCLIFE) : 2. P/E 58 3. Book Value (RS) 23.57Documento5 páginasHDFC Life Insurance (HDFCLIFE) : 2. P/E 58 3. Book Value (RS) 23.57Srini VasanAinda não há avaliações
- Little Ann and Other Poems by Ann Taylor and Jane TaylorDocumento41 páginasLittle Ann and Other Poems by Ann Taylor and Jane Tayloralexa alexaAinda não há avaliações
- Vocab PDFDocumento29 páginasVocab PDFShahab SaqibAinda não há avaliações
- Bi RadsDocumento10 páginasBi RadsFeiky Herfandi100% (1)
- Data Obat VMedisDocumento53 páginasData Obat VMedismica faradillaAinda não há avaliações
- Starters Flash CardsDocumento28 páginasStarters Flash CardsNara GarridoAinda não há avaliações
- Demolition/Removal Permit Application Form: Planning, Property and Development DepartmentDocumento3 páginasDemolition/Removal Permit Application Form: Planning, Property and Development DepartmentAl7amdlellahAinda não há avaliações
- Plastic Omnium 2015 RegistrationDocumento208 páginasPlastic Omnium 2015 Registrationgsravan_23Ainda não há avaliações
- The Effect OfAdditional Nanoparticles Supplementation of Indonesian Bay Leaf (SyzigiumPolyanthum) On Blood Pressure in Pregnancy HypertensionDocumento4 páginasThe Effect OfAdditional Nanoparticles Supplementation of Indonesian Bay Leaf (SyzigiumPolyanthum) On Blood Pressure in Pregnancy HypertensionInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Dynamic Stretching - Stability - Strength.570239Documento2 páginasDynamic Stretching - Stability - Strength.570239Sylvia GraceAinda não há avaliações
- Learning Guide No 5Documento19 páginasLearning Guide No 5Menal JemalAinda não há avaliações
- Sepsis Management UCLA HealthDocumento23 páginasSepsis Management UCLA HealthKomang_JananuragaAinda não há avaliações
- RDG UNIT 2 Skimming Class A 2021Documento17 páginasRDG UNIT 2 Skimming Class A 2021Yuly Rumondang Wulan SiallaganAinda não há avaliações
- Fortune Falls - Lou VaneDocumento402 páginasFortune Falls - Lou VanetesteAinda não há avaliações
- طبى 145Documento2 páginasطبى 145Yazan AbuFarhaAinda não há avaliações
- Marketing ProjectDocumento82 páginasMarketing ProjectSumit GuptaAinda não há avaliações
- Drake Family - Work SampleDocumento1 páginaDrake Family - Work Sampleapi-248366250Ainda não há avaliações
- Work of Asha Bhavan Centre - A Nonprofit Indian Organisation For Persons With DisabilityDocumento10 páginasWork of Asha Bhavan Centre - A Nonprofit Indian Organisation For Persons With DisabilityAsha Bhavan CentreAinda não há avaliações
- Injection Analyzer Electronic Unit enDocumento67 páginasInjection Analyzer Electronic Unit enmayralizbethbustosAinda não há avaliações
- Material: Safety Data SheetDocumento3 páginasMaterial: Safety Data SheetMichael JoudalAinda não há avaliações
- Tryout Consent Form - 2014 - Sign and ReturnDocumento2 páginasTryout Consent Form - 2014 - Sign and ReturnSanjeevan BaraAinda não há avaliações
- Content Map PE & Health 12Documento12 páginasContent Map PE & Health 12RIZZA MEA DOLOSOAinda não há avaliações
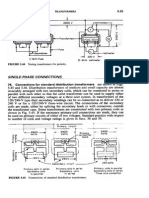
- Transformers ConnectionsDocumento6 páginasTransformers Connectionsgeorgel1980Ainda não há avaliações