Você também pode gostar
- Rotateq Epar Product Information enDocumento29 páginasRotateq Epar Product Information enjjpepAinda não há avaliações
- Leaflet Rotarix Liquid gds15 Ipi11Documento10 páginasLeaflet Rotarix Liquid gds15 Ipi11zeinfahmi16Ainda não há avaliações
- RotaTeq Product Insert PDFDocumento11 páginasRotaTeq Product Insert PDFGea Linggar GalihAinda não há avaliações
- Ocod@fda Hhs GovDocumento14 páginasOcod@fda Hhs Govali subchanAinda não há avaliações
- Adult Immunization ScheduleDocumento3 páginasAdult Immunization ScheduleBryan Mae H. DegorioAinda não há avaliações
- MY VaxigripTetra NH (0522)Documento14 páginasMY VaxigripTetra NH (0522)prasanthgkrishnan1402Ainda não há avaliações
- WHO Position Papers - Recommended Routine Immunizations for ChildrenDocumento8 páginasWHO Position Papers - Recommended Routine Immunizations for Childrenfadityo1Ainda não há avaliações
- Fluvirin Product InsertDocumento13 páginasFluvirin Product InsertShanica Paul-RichardsAinda não há avaliações
- WHO Immunization RecommendationsDocumento9 páginasWHO Immunization RecommendationsMeeKo VideñaAinda não há avaliações
- Practice Changing UpDates - UpToDateDocumento13 páginasPractice Changing UpDates - UpToDatemayteveronica1000Ainda não há avaliações
- ACC_Qdenga_SmPCDocumento18 páginasACC_Qdenga_SmPCAngsamerahAinda não há avaliações
- Adult Pocafeket SizeDocumento2 páginasAdult Pocafeket SizedadfAinda não há avaliações
- HBVAXPRO LeafletDocumento100 páginasHBVAXPRO LeafletEllaAinda não há avaliações
- Nikita Kumari - 2020CH10107 - G14 - 271Documento9 páginasNikita Kumari - 2020CH10107 - G14 - 271Nikita AggarwalAinda não há avaliações
- Adult Immunization Schedule and RecommendationsDocumento3 páginasAdult Immunization Schedule and RecommendationsdrmanojvimalAinda não há avaliações
- WHO Immunization Schedule ChildrenDocumento9 páginasWHO Immunization Schedule Childrenashchua21Ainda não há avaliações
- TAMIFLUDocumento21 páginasTAMIFLUjaphetnwapiAinda não há avaliações
- Adult Combined ScheduleDocumento5 páginasAdult Combined SchedulelcmurilloAinda não há avaliações
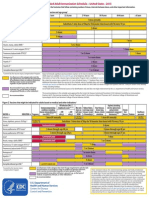
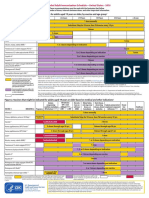
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocumento2 páginasFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasAinda não há avaliações
- Adult ScheduleDocumento3 páginasAdult SchedulelcmurilloAinda não há avaliações
- Children (12 Months To 12 Years of Age)Documento13 páginasChildren (12 Months To 12 Years of Age)doctorkwekkwekAinda não há avaliações
- Wyeth Rotashield Package InsertDocumento19 páginasWyeth Rotashield Package InsertGeeleegoatAinda não há avaliações
- VaricellaDocumento14 páginasVaricellaFaVAinda não há avaliações
- Package Insert VarivaxDocumento13 páginasPackage Insert VarivaxJayantiAinda não há avaliações
- Package Insert - Varivax (Refrigerator)Documento14 páginasPackage Insert - Varivax (Refrigerator)Jose Eduardo Oliva MarinAinda não há avaliações
- VictozaDocumento40 páginasVictozajdkspharmacyAinda não há avaliações
- MolnupiravirDocumento7 páginasMolnupiravirConcepStore PyAinda não há avaliações
- Package Insert - SHINGRIX - 0Documento27 páginasPackage Insert - SHINGRIX - 0fibanezAinda não há avaliações
- Pediatric Gastroenteritis Medication - Vaccines, Antibiotics, AntiemeticsDocumento4 páginasPediatric Gastroenteritis Medication - Vaccines, Antibiotics, AntiemeticsJL CalvinAinda não há avaliações
- Us Infanrix PDFDocumento16 páginasUs Infanrix PDFIrina Fefceac100% (1)
- SOGC Guideline on Immunization in PregnancyDocumento6 páginasSOGC Guideline on Immunization in PregnancyMohamed SulimanAinda não há avaliações
- Tamiflu PDFDocumento28 páginasTamiflu PDFSopheak NGAinda não há avaliações
- Adult Combined ScheduleDocumento5 páginasAdult Combined ScheduleAwal Safar MAinda não há avaliações
- Annex I Summary of Product CharacteristicsDocumento33 páginasAnnex I Summary of Product CharacteristicsVimala BohoAinda não há avaliações
- Linzess Package InsertDocumento21 páginasLinzess Package Insertlorien86Ainda não há avaliações
- Reg 174 Information For Uk Healthcare ProfessionalsDocumento11 páginasReg 174 Information For Uk Healthcare ProfessionalsFranciscoAinda não há avaliações
- Adult Immunization Recommendations SummaryDocumento5 páginasAdult Immunization Recommendations SummaryHannah Caburian RemoAinda não há avaliações
- เอกสารกำกับยา ภาษาอังกฤษ SinovacDocumento12 páginasเอกสารกำกับยา ภาษาอังกฤษ SinovacAtawit SomsiriAinda não há avaliações
- AfinitorDocumento27 páginasAfinitorsvdlindeAinda não há avaliações
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocumento7 páginasTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenKrishnendu PramanikAinda não há avaliações
- Zostavax Epar Product Information - enDocumento46 páginasZostavax Epar Product Information - enArley Miranda CerónAinda não há avaliações
- Nuvaxovid Epar Product Information enDocumento31 páginasNuvaxovid Epar Product Information enKiss TiborAinda não há avaliações
- Adult Schedule 11x17Documento2 páginasAdult Schedule 11x17lcmurilloAinda não há avaliações
- Package Insert - Adenovirus Type 4 and Type 7 Vaccine, Live, Oral - 0Documento14 páginasPackage Insert - Adenovirus Type 4 and Type 7 Vaccine, Live, Oral - 0rampagexoxo79Ainda não há avaliações
- Indian Academy of Pediatrics (IAP) Recommended Immunization Schedule 2013Documento14 páginasIndian Academy of Pediatrics (IAP) Recommended Immunization Schedule 2013Mahesh ShankarAinda não há avaliações
- Full Prescribing Information 1 Indications and UsageDocumento12 páginasFull Prescribing Information 1 Indications and UsageYesika RamirezAinda não há avaliações
- PLENVUDocumento24 páginasPLENVUDuwan ArismendyAinda não há avaliações
- Rota VirusDocumento30 páginasRota VirusboomboompakAinda não há avaliações
- Whole Virion Vaccine InfoDocumento7 páginasWhole Virion Vaccine InfoJoseph Raymund BautistaAinda não há avaliações
- Splenectomy: DisclaimerDocumento5 páginasSplenectomy: DisclaimerMimi FatinAinda não há avaliações
- JR 1Documento32 páginasJR 1berita updateAinda não há avaliações
- Comirnaty Epar Product Information - enDocumento34 páginasComirnaty Epar Product Information - enAuraAinda não há avaliações
- Prospect Prevenar EnglezaDocumento63 páginasProspect Prevenar EnglezaNicoleta CiobotarAinda não há avaliações
- Contraindications and Precautionary Conditions For VaccinatiDocumento25 páginasContraindications and Precautionary Conditions For VaccinatikrishnasreeAinda não há avaliações
- COVID-19 Vaccine AstraZeneca ExplainerDocumento6 páginasCOVID-19 Vaccine AstraZeneca ExplainerBakAinda não há avaliações
- Mounjaro UspiDocumento19 páginasMounjaro UspiayaznptiAinda não há avaliações
- Orig 1 S 031 LBLDocumento11 páginasOrig 1 S 031 LBLNousheenAinda não há avaliações
- Comirnaty Epar Product Information - enDocumento536 páginasComirnaty Epar Product Information - enManaila GabrielAinda não há avaliações
- OsimertinibDocumento16 páginasOsimertinibaziskarnAinda não há avaliações
- CPT® 2015: Watch For Changes in Vertebral Fracture AssessmentDocumento3 páginasCPT® 2015: Watch For Changes in Vertebral Fracture AssessmenttimvrghsAinda não há avaliações
- Bladder Irrigation and InstillationDocumento212 páginasBladder Irrigation and InstillationtimvrghsAinda não há avaliações
- Bariatric SurgeryDocumento5 páginasBariatric SurgerytimvrghsAinda não há avaliações
- Allergen ImmunotherapyDocumento3 páginasAllergen ImmunotherapytimvrghsAinda não há avaliações
- (E.g., Hips, Pelvis, Spine) ) With V82.81 (Special Screening For Osteoporosis)Documento2 páginas(E.g., Hips, Pelvis, Spine) ) With V82.81 (Special Screening For Osteoporosis)timvrghsAinda não há avaliações
- CPT © 2014 American Medical Association. All Rights ReservedDocumento2 páginasCPT © 2014 American Medical Association. All Rights ReservedtimvrghsAinda não há avaliações
- Chapter 1: Anesthesia: Plus: Migraine Revisions Focus On Punctuation Addition, Not Descriptor ChangeDocumento2 páginasChapter 1: Anesthesia: Plus: Migraine Revisions Focus On Punctuation Addition, Not Descriptor ChangetimvrghsAinda não há avaliações
- CPT © 2014 American Medical Association. All Rights ReservedDocumento2 páginasCPT © 2014 American Medical Association. All Rights ReservedtimvrghsAinda não há avaliações
- Multiple) ) - If The Intraoperative Biopsy Reveals Malignancy, The Ob-Gyn May Convert To An Open Procedure To RemoveDocumento2 páginasMultiple) ) - If The Intraoperative Biopsy Reveals Malignancy, The Ob-Gyn May Convert To An Open Procedure To RemovetimvrghsAinda não há avaliações
- CPT © 2014 American Medical Association. All Rights ReservedDocumento2 páginasCPT © 2014 American Medical Association. All Rights ReservedtimvrghsAinda não há avaliações
- Angiography and AortographyDocumento236 páginasAngiography and AortographytimvrghsAinda não há avaliações
- Abdomen and RetroperitoneumDocumento3 páginasAbdomen and RetroperitoneumtimvrghsAinda não há avaliações
- Abdomen X RayDocumento4 páginasAbdomen X RaytimvrghsAinda não há avaliações
- Guide Pdf1471676205 RecoveredDocumento4 páginasGuide Pdf1471676205 RecoveredtimvrghsAinda não há avaliações
- Academic Reading Sample Task Identifying Writers ViewsDocumento4 páginasAcademic Reading Sample Task Identifying Writers ViewsckwasanaAinda não há avaliações
- Website - EX Rate - 02 - Sep - 2016 PDFDocumento1 páginaWebsite - EX Rate - 02 - Sep - 2016 PDFtimvrghsAinda não há avaliações
- DCC Summer 2015Documento12 páginasDCC Summer 2015timvrghsAinda não há avaliações
- Of Intestinal Adhesion) (Separate Procedure) ) Because The Correct Coding Initiative (CCI) Permanently Bundles 44005Documento2 páginasOf Intestinal Adhesion) (Separate Procedure) ) Because The Correct Coding Initiative (CCI) Permanently Bundles 44005timvrghs100% (1)
- 2015 Coding Updates92Documento14 páginas2015 Coding Updates92timvrghsAinda não há avaliações
- 2015 Coding UpdatesDocumento4 páginas2015 Coding UpdatestimvrghsAinda não há avaliações
- Abdomen X RayDocumento4 páginasAbdomen X RaytimvrghsAinda não há avaliações
- Pen TaximDocumento5 páginasPen TaximtimvrghsAinda não há avaliações
- Abortion Diagnosis CodingDocumento3 páginasAbortion Diagnosis CodingtimvrghsAinda não há avaliações
- Infanrix Hexa (Preservative Free) CMI PDF Clean PDFDocumento5 páginasInfanrix Hexa (Preservative Free) CMI PDF Clean PDFtimvrghsAinda não há avaliações
- Canine Fossa.: CPT © 2015 American Medical Association. All Rights ReservedDocumento6 páginasCanine Fossa.: CPT © 2015 American Medical Association. All Rights ReservedtimvrghsAinda não há avaliações
- Aap 2011 Vaccine Coding ChangesDocumento9 páginasAap 2011 Vaccine Coding ChangestimvrghsAinda não há avaliações
- Prevenfdar VaccineDocumento3 páginasPrevenfdar Vaccinetimvrghs123Ainda não há avaliações
- Case Taking SheetDocumento3 páginasCase Taking Sheetssrkm guptaAinda não há avaliações
- Betamethasone Oral Drops for Registered Medical PractitionersDocumento8 páginasBetamethasone Oral Drops for Registered Medical PractitionersAnamika VatsalAinda não há avaliações
- PEGS CatalogDocumento88 páginasPEGS CatalogMAinda não há avaliações
- Harrisons Reviewer Most Common 1Documento59 páginasHarrisons Reviewer Most Common 1Dre Valdez67% (3)
- Coronavirus (COVID-19) RecordsDocumento3 páginasCoronavirus (COVID-19) RecordsTestertAinda não há avaliações
- Operator Loadout for Arid EnvironmentsDocumento11 páginasOperator Loadout for Arid EnvironmentsJustus WeißeAinda não há avaliações
- ASTHMA IN CHILDRENDocumento5 páginasASTHMA IN CHILDRENRenjie ElizardeAinda não há avaliações
- Malaria Managment Algorithm 202208Documento1 páginaMalaria Managment Algorithm 202208Marianne Joy PontigonAinda não há avaliações
- Multiple SclerosisDocumento96 páginasMultiple SclerosisDrGasnasAinda não há avaliações
- Rapid Test For Entamoeba AmoebiasisDocumento3 páginasRapid Test For Entamoeba AmoebiasisWeng Kin WongAinda não há avaliações
- Laboratorio Clinico Parque Escorial: Patient Number Birthdate SexDocumento1 páginaLaboratorio Clinico Parque Escorial: Patient Number Birthdate SexCarol Melissa AquinoAinda não há avaliações
- Presentation CovidDocumento2 páginasPresentation CovidYungfuAinda não há avaliações
- Limfadenopati LimfadenitisDocumento45 páginasLimfadenopati LimfadenitisM Fiqih ArrachmanAinda não há avaliações
- Ministerul Sănătății Vaccination CertificateDocumento1 páginaMinisterul Sănătății Vaccination CertificateКристина ДолотиноваAinda não há avaliações
- Herpes Simplex Genitalia: Pante, Jaselle Paronable, Ana MurielDocumento18 páginasHerpes Simplex Genitalia: Pante, Jaselle Paronable, Ana MurielThea MallariAinda não há avaliações
- Treatment of Sepsis by Extracorporeal Blood Purification SystemsDocumento23 páginasTreatment of Sepsis by Extracorporeal Blood Purification SystemsyamtotlAinda não há avaliações
- Uk PFAPADocumento5 páginasUk PFAPAPrerna SehgalAinda não há avaliações
- Types of VaccinesDocumento2 páginasTypes of VaccinesTamal MannaAinda não há avaliações
- Blood Basics: 1. What Makes Up The Blood in Our Bodies?Documento2 páginasBlood Basics: 1. What Makes Up The Blood in Our Bodies?Jessica StewartAinda não há avaliações
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocumento1 páginaCertificate For COVID-19 Vaccination: Beneficiary DetailsAbdul khadarAinda não há avaliações
- Form Evaluaso AmsDocumento1 páginaForm Evaluaso AmsNadial uzmahAinda não há avaliações
- Atopic Dermatitis Treatment, Pictures, Home Remedies & CausesDocumento19 páginasAtopic Dermatitis Treatment, Pictures, Home Remedies & CausesABHINABA GUPTAAinda não há avaliações
- Zika Virus - CDCDocumento5 páginasZika Virus - CDCLoretta McCalopeAinda não há avaliações
- Subject Plan B.SC Nursing 1 Year: MicrobiologyDocumento2 páginasSubject Plan B.SC Nursing 1 Year: MicrobiologySandeep KumarAinda não há avaliações
- Package Insert Leaflet HbsAg Abbott QuantitativeDocumento7 páginasPackage Insert Leaflet HbsAg Abbott QuantitativeirdinamarchsyaAinda não há avaliações
- CMMC Case - A Diagnostic DilemmaDocumento10 páginasCMMC Case - A Diagnostic DilemmaADIAinda não há avaliações
- Aggressive Periodontitis: Localized & Generalized Forms by SamDocumento24 páginasAggressive Periodontitis: Localized & Generalized Forms by SamNaghman Zuberi100% (1)
- Primary Skin Lesions GuideDocumento39 páginasPrimary Skin Lesions GuideJorelle MarquezAinda não há avaliações
- mRNA Drug ListDocumento48 páginasmRNA Drug ListCarrieAinda não há avaliações
- Activity in Kirby Bauer MethodDocumento2 páginasActivity in Kirby Bauer MethodMaui Vecinal de GuzmanAinda não há avaliações
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeAinda não há avaliações
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementNo EverandTechniques Exercises And Tricks For Memory ImprovementNota: 4.5 de 5 estrelas4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 5 de 5 estrelas5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesNo EverandThe Ultimate Guide To Memory Improvement TechniquesNota: 5 de 5 estrelas5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 5 de 5 estrelas5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 3.5 de 5 estrelas3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNo EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNota: 5 de 5 estrelas5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingNo EverandThe Happiness Trap: How to Stop Struggling and Start LivingNota: 4 de 5 estrelas4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsAinda não há avaliações
- The Tennis Partner: A Doctor's Story of Friendship and LossNo EverandThe Tennis Partner: A Doctor's Story of Friendship and LossNota: 4.5 de 5 estrelas4.5/5 (4)