Você também pode gostar
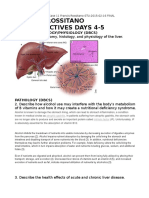
- Francis Rossitano Case Objectives Days 4-5: Anatomy/Histology/Physiology (DBCS)Documento7 páginasFrancis Rossitano Case Objectives Days 4-5: Anatomy/Histology/Physiology (DBCS)Phil BobAinda não há avaliações
- Awareness of Oral Manifestations Related To Systemic DiseasesDocumento5 páginasAwareness of Oral Manifestations Related To Systemic DiseasesInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Gastrointestinal Conditions Related To Tooth Wear: GeneralDocumento4 páginasGastrointestinal Conditions Related To Tooth Wear: Generalfdeetny webassAinda não há avaliações
- Oral Manifestations of Nuritional Diseases in Children1Documento5 páginasOral Manifestations of Nuritional Diseases in Children1andrada67Ainda não há avaliações
- Oral Manifestations of Celiac DiseaseDocumento4 páginasOral Manifestations of Celiac DiseaseAekta PatelAinda não há avaliações
- Pediatric Oral Manifestation of Sustemic DiseaseDocumento43 páginasPediatric Oral Manifestation of Sustemic DiseaseMike SihombingAinda não há avaliações
- Oral, Git, Billiary ConditionsDocumento107 páginasOral, Git, Billiary ConditionsNathaniel Mbiu TimAinda não há avaliações
- Oral Health in Children With Leukemia: Review ArticleDocumento8 páginasOral Health in Children With Leukemia: Review ArticleNindy TweelingenAinda não há avaliações
- Ilovepdf MergedDocumento7 páginasIlovepdf MergedNoval BalanceAinda não há avaliações
- Prevalence of Periodontal Disease in Children With Leukemia and ThalassemiaDocumento14 páginasPrevalence of Periodontal Disease in Children With Leukemia and ThalassemiaZackAinda não há avaliações
- Oral Hygiene Day 2021: Oral Health Care and DiabetesDocumento40 páginasOral Hygiene Day 2021: Oral Health Care and DiabetesAASIM AlamAinda não há avaliações
- Manifestasi Oral No 3 PDFDocumento3 páginasManifestasi Oral No 3 PDFAgum AripratamaAinda não há avaliações
- Cara Perawatan Gigi Tiruan LepasanDocumento3 páginasCara Perawatan Gigi Tiruan LepasanBayyin Bunayya CholidAinda não há avaliações
- Dental Management of Medically Compromised ChildrenDocumento12 páginasDental Management of Medically Compromised Childrenعمار محمد عباسAinda não há avaliações
- 7 Oral Health of Geriatric People Modified Copy or ReferenceDocumento15 páginas7 Oral Health of Geriatric People Modified Copy or ReferenceNitya KrishnaAinda não há avaliações
- 55 Diagnosis, Prevention and Management of Dental ErosionDocumento29 páginas55 Diagnosis, Prevention and Management of Dental Erosionraed ibrahimAinda não há avaliações
- Oral Medicine - Update For The Dental Practitioner.: Dry Mouth and Disorders of SalivationDocumento5 páginasOral Medicine - Update For The Dental Practitioner.: Dry Mouth and Disorders of SalivationGowriAinda não há avaliações
- Oral Candidiasis Causes Types and Treatment PDFDocumento12 páginasOral Candidiasis Causes Types and Treatment PDFTiborAinda não há avaliações
- Silk 2014Documento16 páginasSilk 2014aaAinda não há avaliações
- Oral Manifestations and Complications of Diabetes Mellitus: A ReviewDocumento3 páginasOral Manifestations and Complications of Diabetes Mellitus: A ReviewKiftiyah RahmadhantiAinda não há avaliações
- Ijpi 3 2 75 79Documento5 páginasIjpi 3 2 75 79Rabiatul AdawiyahAinda não há avaliações
- 7 PDFDocumento4 páginas7 PDFAyu Putri Leciyuni TadEsAinda não há avaliações
- Jurnal Diabetes Mellitus Dan Kesehatan MulutDocumento15 páginasJurnal Diabetes Mellitus Dan Kesehatan MulutulfanihanaAinda não há avaliações
- Soalan Temuduga Pegawai PergigianDocumento8 páginasSoalan Temuduga Pegawai PergigianMuhammad Hafizul Amin Bin JimaainAinda não há avaliações
- Oral Frictional HyperkeratosisDocumento15 páginasOral Frictional HyperkeratosisFajarRahmantiyoAinda não há avaliações
- A Review Article of Oral Health and Diabetes Mellitus: Ankita AgarwalDocumento2 páginasA Review Article of Oral Health and Diabetes Mellitus: Ankita Agarwalankita agarwalAinda não há avaliações
- Stomatitis: Overview of The AnatomyDocumento6 páginasStomatitis: Overview of The Anatomyjhing_tajulAinda não há avaliações
- Dental CariesDocumento25 páginasDental CariesFemi100% (1)
- Gastrointestinal Disease in Guinea Pigs and RabbitsDocumento16 páginasGastrointestinal Disease in Guinea Pigs and RabbitsNatali Soto TitoAinda não há avaliações
- Feline Oral DiseasesDocumento6 páginasFeline Oral DiseasesBogdan PopaAinda não há avaliações
- Timbulnya Angular Cheilitis Pada Anak Usia 6Documento9 páginasTimbulnya Angular Cheilitis Pada Anak Usia 6Dona Prima Sari0% (1)
- Preven Lec27Documento6 páginasPreven Lec27Sura Abdel JabbarAinda não há avaliações
- Risk Factors For Periodontal Diseases 2022Documento13 páginasRisk Factors For Periodontal Diseases 2022SnowAinda não há avaliações
- Makalah Modul 1Documento49 páginasMakalah Modul 1gadisestiAinda não há avaliações
- Nutrition in Etentulous PatientsDocumento23 páginasNutrition in Etentulous PatientsKartik R. MorjariaAinda não há avaliações
- Roleof Diabetesin ProsthodonticsDocumento4 páginasRoleof Diabetesin ProsthodonticsHemiya ThomasAinda não há avaliações
- Periodontal Diseases in Children PedoDocumento34 páginasPeriodontal Diseases in Children Pedoarpita7dr9693Ainda não há avaliações
- General DentistryDocumento12 páginasGeneral DentistryCaterina PatrauceanAinda não há avaliações
- Health Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Documento5 páginasHealth Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Kamado NezukoAinda não há avaliações
- Health Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Documento5 páginasHealth Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Kamado NezukoAinda não há avaliações
- More Milk, Stronger Teeth? (Part I)Documento4 páginasMore Milk, Stronger Teeth? (Part I)Nicole StoicaAinda não há avaliações
- Pedodontic Lect 17Documento10 páginasPedodontic Lect 17Mustafa AmmarAinda não há avaliações
- Diagnosis, Prevention and Management of Dental ErosionDocumento29 páginasDiagnosis, Prevention and Management of Dental ErosionDr.Mandeep RallanAinda não há avaliações
- CleftLip StatPearls NCBIBookshelfDocumento6 páginasCleftLip StatPearls NCBIBookshelfDébora QuagliatoAinda não há avaliações
- Articles About DiabetesDocumento10 páginasArticles About DiabetesObed AZARD -Ainda não há avaliações
- Oral Manifestations of Systemic DiseasesDocumento14 páginasOral Manifestations of Systemic Diseasesshygal1981Ainda não há avaliações
- Oral Complications of Cancer TreatmentDocumento68 páginasOral Complications of Cancer TreatmentFarisha RasheedAinda não há avaliações
- Periodontal Disease and Control of Diabetes Mellitus: Clinical PracticeDocumento6 páginasPeriodontal Disease and Control of Diabetes Mellitus: Clinical PracticeOsama HandrAinda não há avaliações
- Dental Management of Medically Compromised PatientsDocumento12 páginasDental Management of Medically Compromised Patientsمحمد ابوالمجدAinda não há avaliações
- Oralhealth in HivDocumento14 páginasOralhealth in HivRochman MujayantoAinda não há avaliações
- Oral Microbiology Periodontitis PDFDocumento85 páginasOral Microbiology Periodontitis PDFSIDNEY SumnerAinda não há avaliações
- Jurnal 3Documento6 páginasJurnal 3Rizki Cah KeratonAinda não há avaliações
- Oral Signs Log of LitDocumento2 páginasOral Signs Log of Litapi-663970258Ainda não há avaliações
- 8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethDocumento8 páginas8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethAhmed AbdAinda não há avaliações
- Ppad Cortellini PDFDocumento9 páginasPpad Cortellini PDFDavid ColonAinda não há avaliações