Você também pode gostar
- FDA Lto ChecklistDocumento4 páginasFDA Lto ChecklistWillard Lucio100% (1)
- Transfer of Medicines SOPDocumento3 páginasTransfer of Medicines SOPPROBLEMSOLVERAinda não há avaliações
- Apply for FDA License to Operate (LTO) in the PhilippinesDocumento3 páginasApply for FDA License to Operate (LTO) in the Philippinesarkina_sunshine0% (1)
- CAPA Plan Farmacia Delim and General MerchandiseDocumento4 páginasCAPA Plan Farmacia Delim and General MerchandiseArianne Courtney Nacar100% (1)
- Standard Operating Procedure Good Storage PracticeDocumento2 páginasStandard Operating Procedure Good Storage PracticeDaniel Yves IV Paez100% (1)
- TR-Pharmacy Services NC IIIDocumento135 páginasTR-Pharmacy Services NC IIIAljon Fortaleza Balanag100% (2)
- Drug Approval System of The Philippines PDFDocumento56 páginasDrug Approval System of The Philippines PDFPatrick OribelloAinda não há avaliações
- Requirements For Opening A Drugstore PDFDocumento2 páginasRequirements For Opening A Drugstore PDFPsyar Lysa Javier100% (2)
- Ppgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityDocumento5 páginasPpgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityIsabel Peralta50% (2)
- Letter of Intent To FDADocumento2 páginasLetter of Intent To FDAGracie Martin100% (1)
- Standard Operating Procedure 4 PDF FreeDocumento19 páginasStandard Operating Procedure 4 PDF FreeMillen100% (2)
- BFADDocumento4 páginasBFADKc Ganda BAinda não há avaliações
- PPGP-Mfg - Receiving Leaflet MaterialDocumento7 páginasPPGP-Mfg - Receiving Leaflet MaterialIsabel EsquijoAinda não há avaliações
- Internship5 12Documento7 páginasInternship5 12Jerel MarquezAinda não há avaliações
- Corrective Action and Preventive Action Plan: RFO/CODocumento3 páginasCorrective Action and Preventive Action Plan: RFO/COMajesty Ymana100% (1)
- Role and Responsibility of Pharmacy Assistant in Community PharmacyDocumento4 páginasRole and Responsibility of Pharmacy Assistant in Community PharmacyUntouchable Monster 2Ainda não há avaliações
- Exercises 8-10 (By Dr. N. Tubon) PDFDocumento25 páginasExercises 8-10 (By Dr. N. Tubon) PDFLoren100% (1)
- NOTES On CDRRHRDocumento8 páginasNOTES On CDRRHRJaica Mangurali TumulakAinda não há avaliações
- Pharmacy SOP: Housekeeping ProceduresDocumento1 páginaPharmacy SOP: Housekeeping ProceduresJaylyne Faith BallogAinda não há avaliações
- Generic drug dispensing process flowDocumento1 páginaGeneric drug dispensing process flowBUPHARCO Mintal Branch100% (1)
- RMP For Drug Establishments - 26 August 2015 PDFDocumento88 páginasRMP For Drug Establishments - 26 August 2015 PDFIan FranklinAinda não há avaliações
- Standard Operating Procedure Pests and Rodents ControlDocumento3 páginasStandard Operating Procedure Pests and Rodents ControlDaniel Yves IV Paez100% (1)
- Railway PharmasistDocumento2 páginasRailway PharmasistprashantAinda não há avaliações
- Westmin Pharmacy - SOPDocumento11 páginasWestmin Pharmacy - SOPJCAsssssiloAinda não há avaliações
- Duties and Responsibilities of PharmacistDocumento3 páginasDuties and Responsibilities of PharmacistChan Orsolino100% (1)
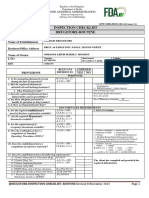
- FDA Inspection Checklist for Sardam Drugstore RoutineDocumento3 páginasFDA Inspection Checklist for Sardam Drugstore RoutineJohanna MonroyAinda não há avaliações
- Personnel Competency EvaluationDocumento4 páginasPersonnel Competency EvaluationMikes Flores100% (1)
- Generic Menu CardDocumento9 páginasGeneric Menu CardLode DeocadesAinda não há avaliações
- RMP For Drug Establishments - 26 August 2015 PDFDocumento88 páginasRMP For Drug Establishments - 26 August 2015 PDFBelle BrionesAinda não há avaliações
- m4 - Check-In Activity 2 (Group #5)Documento6 páginasm4 - Check-In Activity 2 (Group #5)Karren ReyesAinda não há avaliações
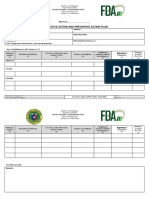
- FDA CAP PlanDocumento3 páginasFDA CAP PlanAlfred John TrinidadAinda não há avaliações
- FDA Philippines E-Portal GuidelinesDocumento37 páginasFDA Philippines E-Portal GuidelinesPeter MifloresAinda não há avaliações
- RegistrationDocumento130 páginasRegistrationJoanne AquinoAinda não há avaliações
- USP43 - NF Acacia SyrupDocumento1 páginaUSP43 - NF Acacia SyrupKhanh Nguyễn PhươngAinda não há avaliações
- GMC Kathua SOP for Pharmacy and Stores ManagementDocumento25 páginasGMC Kathua SOP for Pharmacy and Stores ManagementSauraj GautamAinda não há avaliações
- CRO and Sponsor - Integrated Application FormDocumento4 páginasCRO and Sponsor - Integrated Application FormNaevisweloveuAinda não há avaliações
- Damasco - Cpi - Activity No.9Documento5 páginasDamasco - Cpi - Activity No.9LDCU - Damasco, Erge Iris M.Ainda não há avaliações
- Pharmaceutical SOP ExampleDocumento4 páginasPharmaceutical SOP ExampleFaysal AhmedAinda não há avaliações
- Power Failure Contingency PlanDocumento2 páginasPower Failure Contingency PlanDaniel Yves IV PaezAinda não há avaliações
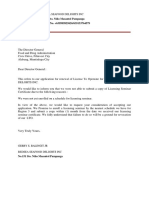
- Redsea Seafood Delights LTO Renewal RequestDocumento1 páginaRedsea Seafood Delights LTO Renewal Requestredseaseafood67% (9)
- Philippines CAP PlanDocumento3 páginasPhilippines CAP PlanCha Gabriel100% (2)
- Generics menu card with pricesDocumento4 páginasGenerics menu card with pricesChris NicodemusAinda não há avaliações
- FDA Labeling RequirementsDocumento50 páginasFDA Labeling RequirementsJean Ganub100% (1)
- DOH-HFSRB-QOP-01-Form 2 A: Print Name and SignatureDocumento1 páginaDOH-HFSRB-QOP-01-Form 2 A: Print Name and SignatureJm Cayabyab0% (1)
- Advocacy in PharmacyDocumento3 páginasAdvocacy in PharmacyZofia RanadaAinda não há avaliações
- 3 Drug Distrubition in HospitalDocumento26 páginas3 Drug Distrubition in HospitalAtrao100% (1)
- Capa Plan 2018Documento3 páginasCapa Plan 2018rainAinda não há avaliações
- Adr-Flow ChartDocumento1 páginaAdr-Flow ChartAJ ArugayAinda não há avaliações
- Cpi - Damasco - Activity 25 & 26Documento3 páginasCpi - Damasco - Activity 25 & 26LDCU - Damasco, Erge Iris M.Ainda não há avaliações
- Pharmacy Services NC IIDocumento50 páginasPharmacy Services NC IIAllan Q VenusAinda não há avaliações
- Standard Operating Procedure Good Dispensing PracticeDocumento2 páginasStandard Operating Procedure Good Dispensing PracticeDaniel Yves IV Paez100% (1)
- Edpms Complete GuideDocumento75 páginasEdpms Complete Guidesheryl GuillermoAinda não há avaliações
- Requirements For Renewal Lto ApplicationDocumento1 páginaRequirements For Renewal Lto ApplicationAnonymous ku7POqvKAinda não há avaliações
- RA 5921 Regulates Pharmacy Practice & Education StandardsDocumento14 páginasRA 5921 Regulates Pharmacy Practice & Education StandardsSunshine_Bacla_4275100% (1)
- Damasco - Cpi - Activity No. 10Documento18 páginasDamasco - Cpi - Activity No. 10LDCU - Damasco, Erge Iris M.Ainda não há avaliações
- 1 - DS SATK Form - Initial Application of LTO 1.1Documento4 páginas1 - DS SATK Form - Initial Application of LTO 1.1Rudejane TanAinda não há avaliações
- 1 DM SATK Form Initial Application of LTODocumento5 páginas1 DM SATK Form Initial Application of LTOkhara teanoAinda não há avaliações
- 3 - DS SATK Form - Change of Ownership 1.2Documento3 páginas3 - DS SATK Form - Change of Ownership 1.2Maybielyn DavidAinda não há avaliações
- 4 - DS SATK Form - Transfer of Location 1.2Documento3 páginas4 - DS SATK Form - Transfer of Location 1.2Maybielyn DavidAinda não há avaliações
- 1 DD SATK Form Initial Application of LTODocumento4 páginas1 DD SATK Form Initial Application of LTOAnonymous i0YU1qCtmAinda não há avaliações
- Bamboo Courses MatrixDocumento2 páginasBamboo Courses Matrixcheska yahniiAinda não há avaliações
- Bamboost ModuleDocumento8 páginasBamboost Modulecheska yahniiAinda não há avaliações
- A Reflection Paper On DepEd CHED and TESDocumento14 páginasA Reflection Paper On DepEd CHED and TEScheska yahniiAinda não há avaliações
- r4f Pastest MnemonicsDocumento23 páginasr4f Pastest MnemonicsplayuhzAinda não há avaliações
- Montgomery County Ten Year Comprehensive Water Supply and Sewerage Systems Plan (2003)Documento228 páginasMontgomery County Ten Year Comprehensive Water Supply and Sewerage Systems Plan (2003)rebolavAinda não há avaliações
- WSAWLD002Documento29 páginasWSAWLD002Nc BeanAinda não há avaliações
- Aphasia PDFDocumento4 páginasAphasia PDFRehab Wahsh100% (1)
- Cement ReportDocumento86 páginasCement ReportSohaibAinda não há avaliações
- Calm Your Aggressive DogDocumento58 páginasCalm Your Aggressive DogASd33475% (4)
- Mabuhay Wedding Package2006Documento3 páginasMabuhay Wedding Package2006Darwin Dionisio ClementeAinda não há avaliações
- Antenna LecDocumento31 páginasAntenna Lecjosesag518Ainda não há avaliações
- g21 Gluta MsdsDocumento3 páginasg21 Gluta Msdsiza100% (1)
- ME JBP 70A Pen Dissolved Oxygen Meter PDFDocumento1 páginaME JBP 70A Pen Dissolved Oxygen Meter PDFpiknikmonsterAinda não há avaliações
- QRF HD785-7Documento2 páginasQRF HD785-7Ralf MaurerAinda não há avaliações
- Stress and FilipinosDocumento28 páginasStress and FilipinosDaniel John Arboleda100% (2)
- Nursing Plan of Care Concept Map - Immobility - Hip FractureDocumento2 páginasNursing Plan of Care Concept Map - Immobility - Hip Fracturedarhuynh67% (6)
- RHS NCRPO COVID FormDocumento1 páginaRHS NCRPO COVID Formspd pgsAinda não há avaliações
- Study On Marketing Strategies of Fast Food Joints in IndiaDocumento35 páginasStudy On Marketing Strategies of Fast Food Joints in IndiaNiveditaParaashar100% (1)
- Quality ImprovementDocumento3 páginasQuality ImprovementViky SinghAinda não há avaliações
- Synthesis, Experimental and Theoretical Characterizations of A NewDocumento7 páginasSynthesis, Experimental and Theoretical Characterizations of A NewWail MadridAinda não há avaliações
- SVIMS-No Que-2Documento1 páginaSVIMS-No Que-2LikhithaReddy100% (1)
- AZ ATTR Concept Test Clean SCREENERDocumento9 páginasAZ ATTR Concept Test Clean SCREENEREdwin BennyAinda não há avaliações
- InjectorDocumento23 páginasInjectorBac Nguyen100% (1)
- Operating Instructions: Katflow 100Documento52 páginasOperating Instructions: Katflow 100Nithin KannanAinda não há avaliações
- Haematology Notes - 3rd EdDocumento100 páginasHaematology Notes - 3rd EdSally Brit100% (1)
- AAR Maintenance 001Documento3 páginasAAR Maintenance 001prakash reddyAinda não há avaliações
- Laboratorio 1Documento6 páginasLaboratorio 1Marlon DiazAinda não há avaliações
- The Danger of Microwave TechnologyDocumento16 páginasThe Danger of Microwave Technologyrey_hadesAinda não há avaliações
- Reading and Listening 2Documento4 páginasReading and Listening 2Hải Anh TạAinda não há avaliações
- Natural Resources in PakistanDocumento5 páginasNatural Resources in PakistanSohaib EAinda não há avaliações
- BCM Continuous ImprovementDocumento22 páginasBCM Continuous ImprovementnikoAinda não há avaliações
- Human Capital FormationDocumento9 páginasHuman Capital Formationtannu singh67% (6)
- HVDC BasicDocumento36 páginasHVDC BasicAshok KumarAinda não há avaliações
- Analisis Dampak Reklamasi Teluk Banten Terhadap Kondisi Lingkungan Dan Sosial EkonomiDocumento10 páginasAnalisis Dampak Reklamasi Teluk Banten Terhadap Kondisi Lingkungan Dan Sosial EkonomiSYIFA ABIYU SAGITA 08211840000099Ainda não há avaliações