Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Dna VirusDocumento3 páginasDna VirusMaisie LeeAinda não há avaliações
- Arterial-Venous Tree OverviewDocumento5 páginasArterial-Venous Tree OverviewMaisie LeeAinda não há avaliações
- Pregnancy Risks and Breastfeeding PreparationDocumento1 páginaPregnancy Risks and Breastfeeding PreparationMaisie LeeAinda não há avaliações
- App13 PDFDocumento12 páginasApp13 PDFMaisie LeeAinda não há avaliações
- Developing Bone of NailsDocumento3 páginasDeveloping Bone of NailsMaisie LeeAinda não há avaliações
- HallmarksDocumento6 páginasHallmarksMaisie LeeAinda não há avaliações
- Carbohydrate Digestion and Metabolism ExplainedDocumento116 páginasCarbohydrate Digestion and Metabolism ExplainedMaisie LeeAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Bhattacharya S K Short Cases in Surgery PDFDocumento346 páginasBhattacharya S K Short Cases in Surgery PDFRadhika M100% (5)
- Neck MassDocumento13 páginasNeck MassY3153NSAinda não há avaliações
- PracticalDocumento89 páginasPracticalAthEer AhmadAinda não há avaliações
- Oral Pathology: Non-Epithelialized Primary Bone CystDocumento4 páginasOral Pathology: Non-Epithelialized Primary Bone Cystعلي صادق جعفرAinda não há avaliações
- ENT - Essays - Sun 2016Documento6 páginasENT - Essays - Sun 2016rabeca johnsonAinda não há avaliações
- Neck LumpsDocumento27 páginasNeck LumpsArifudin Cipto HusodoAinda não há avaliações
- CGHS Rates for Medical Procedures in BangaloreDocumento23 páginasCGHS Rates for Medical Procedures in BangaloreVasu RathodAinda não há avaliações
- PEDIATRIC SURGERY PROBLEMSDocumento141 páginasPEDIATRIC SURGERY PROBLEMSsedaka26100% (4)
- A Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressDocumento299 páginasA Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressHamza Khan100% (1)
- Pre Exam Surgical Notes 2Documento166 páginasPre Exam Surgical Notes 2flor vickyAinda não há avaliações
- Journal ENT - Journal - 2008Documento132 páginasJournal ENT - Journal - 2008Furqan MirzaAinda não há avaliações
- Neck Lump HistoryDocumento4 páginasNeck Lump HistoryAlmomnbllah Ahmed100% (1)
- Congenital Neck MassesDocumento9 páginasCongenital Neck Massesjuita auglinaAinda não há avaliações
- Imaging of Cystic or Cyst-Like Neck MassesDocumento10 páginasImaging of Cystic or Cyst-Like Neck MassesRini RahmawulandariAinda não há avaliações
- Masa CervicalDocumento9 páginasMasa CervicalMdacAinda não há avaliações
- Anatomy Head Neck EMRCS MCQDocumento23 páginasAnatomy Head Neck EMRCS MCQTowhid HasanAinda não há avaliações
- Neck SwellingDocumento41 páginasNeck SwellingMahindra Kumar100% (3)
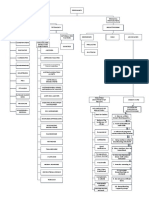
- Thyroid Diseases Embryology, Anatomy, Investigations and TreatmentDocumento41 páginasThyroid Diseases Embryology, Anatomy, Investigations and TreatmentUday Kumar KolluriAinda não há avaliações
- Mojahid Sheet Complete PDFDocumento176 páginasMojahid Sheet Complete PDFOsman SomiAinda não há avaliações
- Evaluation and Management of Neck MassesDocumento38 páginasEvaluation and Management of Neck MassesShaxawan Mahmood AliAinda não há avaliações
- Case Sudy:: Thyroglossal Duct CystDocumento21 páginasCase Sudy:: Thyroglossal Duct CystHope SerquiñaAinda não há avaliações
- Ent Ospe Badhahin v1 7 PDFDocumento26 páginasEnt Ospe Badhahin v1 7 PDFWasi OsmanAinda não há avaliações
- Sistrunk Operation ArticleDocumento4 páginasSistrunk Operation Articleআবু আব্দুল্লাহ শাদীদAinda não há avaliações
- Short Cases and Skill Lab. Sessions in SurgeryDocumento73 páginasShort Cases and Skill Lab. Sessions in SurgeryBiph BiphAinda não há avaliações
- Linfadenopatia Cervical 2018 PediatricsDocumento13 páginasLinfadenopatia Cervical 2018 PediatricsCarlos VegaAinda não há avaliações
- Short Notes and Short Cases in SurgeryDocumento243 páginasShort Notes and Short Cases in SurgeryIosub Lica-Claudiu100% (3)
- Thyroglossal CystsDocumento4 páginasThyroglossal CystsCondurache Ilie-AndreiAinda não há avaliações
- Advanced TUS 2017 Syllabus - SECUREDDocumento373 páginasAdvanced TUS 2017 Syllabus - SECUREDYav KAinda não há avaliações
- Trans SaVi Oto Lec 10 Head and Neck Anatomy and Benign Masses 1st SemDocumento7 páginasTrans SaVi Oto Lec 10 Head and Neck Anatomy and Benign Masses 1st SemJoherAinda não há avaliações
- Chapter 24 Cysts of The Oral and Maxillofacial RegionDocumento47 páginasChapter 24 Cysts of The Oral and Maxillofacial RegionJj JungAinda não há avaliações