Você também pode gostar
- Presbycusis, (Age-related hearing loss) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandPresbycusis, (Age-related hearing loss) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- A Simple Guide to Lows and Highs of Hearing Disorders, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Lows and Highs of Hearing Disorders, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Mineire'sDocumento16 páginasMineire'sShaykh Evangelista BacualAinda não há avaliações
- Effective Ways To Stop SnoringDocumento32 páginasEffective Ways To Stop SnoringKwadwo Baah TiekuAinda não há avaliações
- What Is Presbycusis?: OtosclerosisDocumento8 páginasWhat Is Presbycusis?: OtosclerosisIndraRukmanaHamimPartIIAinda não há avaliações
- Vocal Cord ParalysisDocumento3 páginasVocal Cord ParalysisVenkatesan VidhyaAinda não há avaliações
- GOTB - Group 7 - Geriatric WorldDocumento3 páginasGOTB - Group 7 - Geriatric WorldReza Afif FebriansyahAinda não há avaliações
- Seminar 5 MG IIDocumento6 páginasSeminar 5 MG IIrussianangelAinda não há avaliações
- Hearing Loss (Deafness), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandHearing Loss (Deafness), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNota: 4 de 5 estrelas4/5 (1)
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsAinda não há avaliações
- Anatomy and Physiology of The EarDocumento6 páginasAnatomy and Physiology of The EarrizzarAinda não há avaliações
- Anatomy of Human EarDocumento5 páginasAnatomy of Human EarSharanz Twentyfour SevenAinda não há avaliações
- 683 2Documento15 páginas683 2M Noaman AkbarAinda não há avaliações
- Hearing ImpairementDocumento8 páginasHearing ImpairementMARY KENNETH SILVOSAAinda não há avaliações
- Sensorineural Hearing LossDocumento19 páginasSensorineural Hearing LossBenitaAinda não há avaliações
- Ingles - 1° AñoDocumento43 páginasIngles - 1° AñoRox Sof100% (1)
- Ijsrp p1486Documento6 páginasIjsrp p1486Sandeep KumarAinda não há avaliações
- Your Guide To Better Hearing. VisitDocumento32 páginasYour Guide To Better Hearing. VisitPhonac Hearing CentreAinda não há avaliações
- A Simple Guide to Voice Disorders, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Voice Disorders, Diagnosis, Treatment and Related ConditionsNota: 5 de 5 estrelas5/5 (1)
- ClutteringhandoutDocumento66 páginasClutteringhandoutSiha SalamAinda não há avaliações
- Motor Neuron Disease.Documento38 páginasMotor Neuron Disease.sanjana sangleAinda não há avaliações
- Psych 16Documento73 páginasPsych 16rbm121415chyAinda não há avaliações
- Tinnitus Cure Guide: The Ultimate Tinnitus Miracle Cure & Relief GuideNo EverandTinnitus Cure Guide: The Ultimate Tinnitus Miracle Cure & Relief GuideNota: 3.5 de 5 estrelas3.5/5 (9)
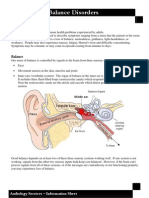
- Dizziness and Balance DisordersDocumento4 páginasDizziness and Balance DisordersEcaterina ChiriacAinda não há avaliações
- Hearing Disorders and Audiogram InterpretationDocumento27 páginasHearing Disorders and Audiogram InterpretationGaluhAinda não há avaliações
- Migraine - More Than A HeadacheDocumento11 páginasMigraine - More Than A HeadacheLuma De Fátima Louro AitaAinda não há avaliações
- Sleep ApnoeaDocumento5 páginasSleep ApnoeaBianca BinnsAinda não há avaliações
- Nursing 1 - Workshop 6Documento9 páginasNursing 1 - Workshop 6GINA NAYIBTH LEON VIDALAinda não há avaliações
- Tinnitus 101 What You Absolutely Need To Know About TinnitusDocumento13 páginasTinnitus 101 What You Absolutely Need To Know About TinnitusivarnorAinda não há avaliações
- Obstructive Sleep ApneaDocumento47 páginasObstructive Sleep ApneaAnusha Ks100% (1)
- Cerebral Palsy: Recommended ReadingDocumento5 páginasCerebral Palsy: Recommended ReadingJoey Ivan CristobalAinda não há avaliações
- PresbycusisDocumento5 páginasPresbycusisdarsunaddictedAinda não há avaliações
- NCM 114 Module 3Documento30 páginasNCM 114 Module 3leinneleinneAinda não há avaliações
- Hearing LossDocumento31 páginasHearing LossDat boi100% (1)
- Ayurveda SadhanaDocumento5 páginasAyurveda SadhanaPRaoAinda não há avaliações
- Reporter: Degenerative Diseases of The Central Nervous System (CNS) Parkinson's DiseaseDocumento6 páginasReporter: Degenerative Diseases of The Central Nervous System (CNS) Parkinson's DiseaseMelody B. MiguelAinda não há avaliações
- Special Sensors PDFDocumento45 páginasSpecial Sensors PDFSwarna JayarathnaAinda não há avaliações
- The Different Types of Sleeping DisordersDocumento5 páginasThe Different Types of Sleeping DisordersRadee King CorpuzAinda não há avaliações
- Muscle TensionDocumento6 páginasMuscle TensionFabián Basaes OlmosAinda não há avaliações
- Migraine Patient HandoutDocumento14 páginasMigraine Patient HandoutthiautamiAinda não há avaliações
- Name: Ericka Vanessa MoránDocumento6 páginasName: Ericka Vanessa MoránLitopez YepezAinda não há avaliações
- Reporting ScienceDocumento20 páginasReporting ScienceYasuhiro Hinggo EscobilloAinda não há avaliações
- Ncm-116-Auditory-Disturbances 2Documento24 páginasNcm-116-Auditory-Disturbances 2aaaawakandaAinda não há avaliações
- Deafness: Lahore College For Women UniversityDocumento25 páginasDeafness: Lahore College For Women Universityjames_sk8734Ainda não há avaliações
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- PD WRDocumento20 páginasPD WRepeydenfajardoAinda não há avaliações
- Protect Your HearingDocumento5 páginasProtect Your HearingReza MahmoudiAinda não há avaliações
- 12 Critical QuestionsDocumento2 páginas12 Critical QuestionsramopavelAinda não há avaliações
- DD PresbikusisDocumento3 páginasDD PresbikusisJ KrystalAinda não há avaliações
- What Is PresbycusisDocumento4 páginasWhat Is PresbycusisNisa UcilAinda não há avaliações
- Natural Remedies That Will Make You or Loved One Stop Snoring Once and for AllNo EverandNatural Remedies That Will Make You or Loved One Stop Snoring Once and for AllAinda não há avaliações
- Classification: Dysarthria ('Dys' Meaning 'Having A Problem With' 'Arthr' Meaning 'Articulating') Is ADocumento3 páginasClassification: Dysarthria ('Dys' Meaning 'Having A Problem With' 'Arthr' Meaning 'Articulating') Is AAppas SahaAinda não há avaliações
- A Simple Guide to Dysphonia, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Dysphonia, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Biology Investigatory Project: Topic: Parkinson'S DiseaseDocumento18 páginasBiology Investigatory Project: Topic: Parkinson'S DiseaseAneesh MoosaAinda não há avaliações
- Disease and Disorder of Nervous SystemDocumento11 páginasDisease and Disorder of Nervous SystemHannah ۦۦAinda não há avaliações
- Parkinson's DiseaseDocumento11 páginasParkinson's Diseaseleeyan2wenty6100% (3)
- Chapter 26: Fluid, Electrolyte & PH Balance: I. Body FluidsDocumento2 páginasChapter 26: Fluid, Electrolyte & PH Balance: I. Body FluidsJohn OmandacAinda não há avaliações
- FAPA ProgrammeDocumento1 páginaFAPA ProgrammeJohn OmandacAinda não há avaliações
- Vol1-No2-1 Farming PDFDocumento4 páginasVol1-No2-1 Farming PDFRania GaneshaAinda não há avaliações
- Allegations PDFDocumento34 páginasAllegations PDFJohn Omandac100% (1)
- Chapter 26: Fluid, Electrolyte & PH Balance: I. Body FluidsDocumento2 páginasChapter 26: Fluid, Electrolyte & PH Balance: I. Body FluidsJohn OmandacAinda não há avaliações
- BF 02493214Documento2 páginasBF 02493214John OmandacAinda não há avaliações
- Doi - Article Id 10.5530ijper.51.3s.30Documento5 páginasDoi - Article Id 10.5530ijper.51.3s.30John OmandacAinda não há avaliações
- Personnel Metrics PDFDocumento65 páginasPersonnel Metrics PDFJohn OmandacAinda não há avaliações
- IJPC 21-1-39 Basics-Of-Compounding HumcoDocumento7 páginasIJPC 21-1-39 Basics-Of-Compounding HumcoJohn OmandacAinda não há avaliações
- Analysis of Bisphenol A in Blood and Urine SamplesDocumento5 páginasAnalysis of Bisphenol A in Blood and Urine SamplesJohn OmandacAinda não há avaliações
- Emergency Preparedness QuizDocumento6 páginasEmergency Preparedness QuizJakie UbinaAinda não há avaliações
- Carbopol PolymersDocumento6 páginasCarbopol Polymersdidimik100% (3)
- Laboratory Manual Pesticide CompleteDocumento53 páginasLaboratory Manual Pesticide CompleteJohn OmandacAinda não há avaliações
- Nmpha-Sible-Usp797 and Usp 800Documento44 páginasNmpha-Sible-Usp797 and Usp 800John OmandacAinda não há avaliações
- National Library of The Philippines Online Public Access Catalog Catalog - Details For: Philippine Pharmaceutical Law, Jurisprudence and EthicsDocumento1 páginaNational Library of The Philippines Online Public Access Catalog Catalog - Details For: Philippine Pharmaceutical Law, Jurisprudence and EthicsJohn OmandacAinda não há avaliações
- Doi - Article Id 10.5530ijper.51.3s.30Documento5 páginasDoi - Article Id 10.5530ijper.51.3s.30John OmandacAinda não há avaliações
- Kakatiya University, Warangal: Department of Pharmaceutics University College of Pharmaceutical SciencesDocumento27 páginasKakatiya University, Warangal: Department of Pharmaceutics University College of Pharmaceutical SciencesJohn OmandacAinda não há avaliações
- FAPA ProgrammeDocumento1 páginaFAPA ProgrammeJohn OmandacAinda não há avaliações
- CosentyxDocumento32 páginasCosentyxJohn OmandacAinda não há avaliações
- Brand GuidelinesDocumento45 páginasBrand GuidelinesJohn OmandacAinda não há avaliações
- Rule Iii Implementing Rules and Regulations of The Philippine Pharmacy Act of 2016Documento1 páginaRule Iii Implementing Rules and Regulations of The Philippine Pharmacy Act of 2016John OmandacAinda não há avaliações
- ELSIDocumento22 páginasELSIJohn OmandacAinda não há avaliações
- AgarDocumento2 páginasAgarJohn OmandacAinda não há avaliações
- Classroom Debate For JurisprudenceDocumento13 páginasClassroom Debate For JurisprudenceJohn OmandacAinda não há avaliações
- TB 2 FollowupDocumento1 páginaTB 2 FollowupJohn OmandacAinda não há avaliações
- InformedConsent ClinicalstudiesDocumento10 páginasInformedConsent ClinicalstudiestisconAinda não há avaliações
- Neiserria GonorrhoeaDocumento1 páginaNeiserria GonorrhoeaJohn OmandacAinda não há avaliações
- HelminthDocumento1 páginaHelminthJohn OmandacAinda não há avaliações
- MentholDocumento2 páginasMentholJohn OmandacAinda não há avaliações
- White Coat HypertensionDocumento7 páginasWhite Coat HypertensionarfikAinda não há avaliações
- Pricing Reimbursement of Drugs and Hta Policies in FranceDocumento20 páginasPricing Reimbursement of Drugs and Hta Policies in FranceHananAhmedAinda não há avaliações
- You Are Dangerous To Your Health CRAWFORDDocumento18 páginasYou Are Dangerous To Your Health CRAWFORDGonzalo PaezAinda não há avaliações
- Advanced EndodonticsDocumento375 páginasAdvanced EndodonticsSaleh Alsadi100% (1)
- Magnesium SulphateDocumento9 páginasMagnesium SulphateNatália A. OliveiraAinda não há avaliações
- Concept of PreventionDocumento48 páginasConcept of Preventionmahmoud100% (1)
- XII - Zool Ch4 REPRODUCTIVE HEALTH Hsslive PDFDocumento4 páginasXII - Zool Ch4 REPRODUCTIVE HEALTH Hsslive PDFPrituAinda não há avaliações
- ResearchDocumento19 páginasResearchKeVongPugehAinda não há avaliações
- Anti Dumping DietDocumento3 páginasAnti Dumping DietFelixDrummaruAinda não há avaliações
- s8. Partograph. ExerciseDocumento44 páginass8. Partograph. ExerciseAngel ReyesAinda não há avaliações
- Importance of Learning Islamic HistoryDocumento102 páginasImportance of Learning Islamic HistoryAnees MohammedAinda não há avaliações
- Perioperative Patient CareDocumento6 páginasPerioperative Patient CareClark LlameraAinda não há avaliações
- NCP AppendicitisDocumento8 páginasNCP AppendicitisAaron_Kim_Vela_4636Ainda não há avaliações
- General Principles of Fracture ManagementDocumento60 páginasGeneral Principles of Fracture ManagementAdrian Joel Quispe AlataAinda não há avaliações
- 1238-Article Text-5203-1-10-20220916Documento3 páginas1238-Article Text-5203-1-10-20220916srirampharmAinda não há avaliações
- Alemnesh MandeshDocumento94 páginasAlemnesh MandeshDAinda não há avaliações
- The Smart Chiropractor A Guide To Marketing Your PracticeDocumento43 páginasThe Smart Chiropractor A Guide To Marketing Your PracticeAaron DriverAinda não há avaliações
- Bionic EyeDocumento20 páginasBionic EyeMegha BhatiaAinda não há avaliações
- Pediatric Head Trauma: PathophysiologyDocumento5 páginasPediatric Head Trauma: Pathophysiologyherman76Ainda não há avaliações
- BurnsDocumento27 páginasBurnsThao TranAinda não há avaliações
- 665 - Assignment 2Documento6 páginas665 - Assignment 2poojaAinda não há avaliações
- SHD Form 4 T - NTPDocumento3 páginasSHD Form 4 T - NTPElle RochAinda não há avaliações
- Insan Anatomisi Atlasi Mcminn 1515167549Documento18 páginasInsan Anatomisi Atlasi Mcminn 1515167549Müslüm ŞahinAinda não há avaliações
- Mariana Katkout, Health Psychology 7501PSYSCI (AP1) A Defense of The Biopsychosocial Model vs. The Biomedical ModelDocumento13 páginasMariana Katkout, Health Psychology 7501PSYSCI (AP1) A Defense of The Biopsychosocial Model vs. The Biomedical ModelMariana KatkoutAinda não há avaliações
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Documento43 páginas(Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Haider Nadhem AL-rubaiAinda não há avaliações
- Comparison of Intravitreal Bevacizumab (Avastin) With Triamcinolone For Treatment of Diffused Diabetic Macular Edema: A Prospective Randomized StudyDocumento9 páginasComparison of Intravitreal Bevacizumab (Avastin) With Triamcinolone For Treatment of Diffused Diabetic Macular Edema: A Prospective Randomized StudyBaru Chandrasekhar RaoAinda não há avaliações
- Soal Bahasa Inggris Kelompok 8 DoneDocumento5 páginasSoal Bahasa Inggris Kelompok 8 Doneputri dwi lailikaAinda não há avaliações
- 2011 Complete Journals Catalog (Incl Open Access Journals)Documento292 páginas2011 Complete Journals Catalog (Incl Open Access Journals)mourighoshAinda não há avaliações
- Eating Disorders: by Pius KigamwaDocumento20 páginasEating Disorders: by Pius KigamwaRahul Kumar DiwakarAinda não há avaliações
- Bombay Hospital InformationBookletDocumento12 páginasBombay Hospital InformationBookletmilkywayAinda não há avaliações