Escolar Documentos
Profissional Documentos
Cultura Documentos
Read Et Al 2009 PDF
Enviado por
Jana ChihaiTítulo original
Direitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
Read Et Al 2009 PDF
Enviado por
Jana ChihaiDireitos autorais:
Formatos disponíveis
Globalization and Health
BioMed Central
Open Access
Research
Local suffering and the global discourse of mental health and human
rights: An ethnographic study of responses to mental illness in rural
Ghana
Ursula M Read1, Edward Adiibokah*2 and Solomon Nyame2
Address: 1Department of Anthropology, University College London, UK and 2Kintampo Health Research Centre, Kintampo, Brong Ahafo, Ghana
Email: Ursula M Read - u.read@ucl.ac.uk; Edward Adiibokah* - adiiboka@yahoo.com; Solomon Nyame - meronzi12345@yahoo.com
* Corresponding author
Published: 14 October 2009
Globalization and Health 2009, 5:13
doi:10.1186/1744-8603-5-13
Received: 28 May 2009
Accepted: 14 October 2009
This article is available from: http://www.globalizationandhealth.com/content/5/1/13
2009 Read et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: The Global Movement for Mental Health has brought renewed attention to the
neglect of people with mental illness within health policy worldwide. The maltreatment of the
mentally ill in many low-income countries is widely reported within psychiatric hospitals, informal
healing centres, and family homes. International agencies have called for the development of
legislation and policy to address these abuses. However such initiatives exemplify a top-down
approach to promoting human rights which historically has had limited impact at the level of those
living with mental illness and their families.
Methods: This research forms part of a longitudinal anthropological study of people with severe
mental illness in rural Ghana. Visits were made to over 40 households with a family member with
mental illness, as well as churches, shrines, hospitals and clinics. Ethnographic methods included
observation, conversation, semi-structured interviews and focus group discussions with people
with mental illness, carers, healers, health workers and community members.
Results: Chaining and beating of the mentally ill was found to be commonplace in homes and
treatment centres in the communities studied, as well as with-holding of food ('fasting'). However
responses to mental illness were embedded within spiritual and moral perspectives and such
treatment provoked little sanction at the local level. Families struggled to provide care for severely
mentally ill relatives with very little support from formal health services. Psychiatric services were
difficult to access, particularly in rural communities, and also seen to have limitations in their
effectiveness. Traditional and faith healers remained highly popular despite the routine
maltreatment of the mentally ill in their facilities.
Conclusion: Efforts to promote the human rights of those with mental illness must engage with
the experiences of mental illness within communities affected in order to grasp how these may
underpin the use of practices such as mechanical restraint. Interventions which operate at the local
level with those living with mental illness within rural communities, as well as family members and
healers, may have greater potential to effect change in the treatment of the mentally ill than
legislation or investment in services alone.
Page 1 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
Background
The contribution of mental disorders to the burden of
chronic disease has been re-affirmed in the latest update
to the Global Burden of Disease (GBD) study. This identifies neuropsychiatric conditions including depression,
psychoses and alcohol use disorders, as the leading causes
of disability worldwide, representing a third of all years of
healthy life lost to disability among adults [1]. According
to this study, the burden of disability is highest in African
countries, presumably due to the impact of poverty and
low levels of treatment and rehabilitation for chronic diseases. Within sub-Saharan Africa the majority of those
with mental disorders receive no treatment from mental
health services. In a study in Nigeria, for example, only
9% of 1,682 people diagnosed with anxiety, mood or substance use disorder had received any treatment, and even
this treatment was judged to be inadequate [2]. Mental
health care is underfunded across the continent compared
to other health concerns. According to the World Health
Organization (WHO), 70% of African countries spend
less than 1% of their health budgets on mental health [3].
Even then the majority of government funding for mental
health is consumed in maintaining large psychiatric institutions, with very little allocated for the treatment and
prevention of mental disorders in the community. In
common with general health care and other public services, psychiatric services tend to be concentrated within
the urban centres of most countries of sub-Saharan Africa.
This means that the poorest members of these countries
who live in rural areas far from the capitals and major cities face the greatest challenges in accessing mental health
care.
In response to these deficits in mental healthcare, 2008
witnessed the launch of The Global Movement for Mental
Health http://www.globalmentalhealth.org. The movement has three key objectives: the scaling up of mental
health services, protecting human rights, and promoting
research in low- and middle-income countries. This
movement is the latest development in a global push for
improved mental health care which began in 2001 with
the World Health Report on mental health [4]. It received
renewed impetus in 2007 with the publication of the Lancet series on mental health which highlighted the paucity
of attention to mental health in the global public health
forum culminating in a 'call for action' [5]. This call,
which forms the foundation of the Global Movement for
Mental Health, suggests that Government ministries
should 'identify and scale up a priority package of service
interventions or components that can form the backbone
of a national mental health system that provides effective
interventions and human-rights protection' [5]. Recommended strategies are in line with long-standing recommendations for the delivery of mental health care which
emphasize the need for decentralisation, community-
http://www.globalizationandhealth.com/content/5/1/13
based mental health care, and the integration of mental
health within primary care. The movement also suggests
that governments of low- and middle-income countries
should establish a national body to monitor and protect
the human rights of people with mental disorders, and
'promote adoption and implementation of national mental health legislation in accordance with international
human-rights instruments' [5]. However this focus on
state interventions to promote human rights faces additional challenges in countries with emerging economies,
and weak systems of governance and civil participation.
Many governments of sub-Saharan Africa for example,
have historically shown little respect for the human rights
of their populations, whether mentally ill or otherwise.
This paper considers the challenges facing the protection
of the human rights of people with mental illness drawing
on the results of ethnographic research in Kintampo, a
rural community in Ghana, West Africa.
Mental health and human rights
Reports by NGOs and the media regarding the widespread
maltreatment of the mentally in low-income countries of
sub-Saharan Africa, including graphic images of people in
chains, have provoked shock and outrage amongst many
observers, and led to urgent calls for reform. It is striking
that such appeals have generally come not from the communities affected, but from concerned visitors and experts
from the international scene - NGOs, WHO and internationally prominent psychiatrists. These concerns are far
from new. In 1991 the UN adopted the 'Principles for the
Protection of Persons with Mental Illness and for the
Improvement for Mental Health Care' (commonly known
as the MI Principles) [6]. In response to the lack of
progress in meeting the minimum standards enshrined in
these principles, the Institute of Psychiatry in the UK
launched 'Principles to Respect', an 'Initiative on Mental
Health and Human Rights' which aimed to promote the
MI principles within psychiatric facilities worldwide [7].
Most recently the UN Convention on the Rights of Persons with Disabilities (including within this definition
those with 'mental impairments') was passed in 2006,
although it remains to be ratified by many countries [8].
All these initiatives draw on the principles of human
rights to prohibit the unlawful deprivation of liberty and
the use of 'cruel, inhuman or degrading treatment or punishment'. Countries are supported by international agencies such as WHO to develop mental health legislation
and policy as a step to improved services and the outlawing of human rights abuses [9]. However, despite the best
intentions of these initiatives, such 'top-down'
approaches are in danger of failing to bring about change
in the communities most affected, as evidenced by the
persistence of human rights abuses in states which have
been signatory to international treaties and conventions,
Page 2 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
as well as reproducing human rights rhetoric within their
national constitutions and legislation. As observed elsewhere, a proliferation of human rights documents has not
correlated with a decrease in human rights abuses [10].
The stark fact remains that in spite of decades of international human rights initiatives, throughout many countries of sub-Saharan Africa the chaining and other
maltreatment of the mentally ill remains routine.
It is perhaps unsurprising that human rights abuses are
often linked to poor standards of mental health care in
low-income countries and the need for methods of
restraint in the absence of easily available neuroleptics.
Data produced by WHO such as the Mental Health Atlas
[3], in which the scarcity of psychiatric resources such as
hospital beds, psychiatrists and mental health spending in
sub-Saharan Africa is all too clear, would seem to support
this conclusion. However such data fails to enumerate the
contributions of family members and religious healers, as
well as other informal resources, which form the backbone of care for the mentally ill in many countries of subSaharan Africa. In addition, attitudes to the care of those
with mental illness seem to vary even between countries
with similar levels of economic development. Whilst
chaining of the mentally ill is commonplace in countries
of sub-Saharan Africa, in Peru this does not occur, even in
remote rural communities where psychiatric services are
scarce (David Orr, University College London, personal
communication). This suggests that responses to the mental illness of a family member are influenced by social
norms regarding the control of mental illness which are in
turn informed by historical, cultural and symbolic practices. Such social norms become the accepted, even
expected, practices in response to mental illness, and
hence may not evoke widespread protest, particularly at
the community level.
This paper draws on anthropological research with people
with mental illness, their families and healing practitioners within rural communities in Ghana, to gain an understanding of how practices such as the chaining and
beating of those with mental illness are embedded within
sociocultural meanings and responses evoked by madness
or mental illness. An ethnographic approach involving
long-term research within the field permits one to trace
the trajectory of family responses to mental illness in
which chaining often forms part of a long period of helpseeking. This research enabled encounters with families
before, during and after the use of chains, and was thus
able to track changes in family responses over time.
Mental health policy and service delivery in Ghana
Like many countries of sub-Saharan Africa, Ghana's psychiatric services have their origins in the colonial period
with the establishment of an asylum in the capital, Accra.
This was largely custodial rather than therapeutic in func-
http://www.globalizationandhealth.com/content/5/1/13
tion and served to detain those with mental illness who
had increasingly come to the notice of the colonial
authorities, particularly in urban areas [11]. Two further
psychiatric hospitals were established following independence offering inpatient and outpatient treatment for
mental disorders. All three hospitals are located in the
south of the country and from their inception have suffered from overcrowding and understaffing leading to
poor quality of care. Despite several initiatives to improve
mental health services, including the training of community psychiatric nurses and the opening of regional psychiatric units, the vision of a comprehensive community
mental health system held by the first African psychiatrist
in the country, E.M. Forster [12], has yet to be fulfilled.
Political apathy towards mental health, combined with
widespread stigma, hamper the progress of mental health
care in the country. Traditional healers, and increasingly
pastors of the Pentecostal churches, continue to deal with
the greatest proportion of those with mental disorders.
Whilst these often address the spiritual concerns of Ghanaians who use their services, there are reports of maltreatment and human rights abuse including chaining,
enforced fasting, and beatings [13].
However there are some signs of a renewed impetus for
mental health care within Ghana. A new mental health
bill has been highly praised for its focus on human rights
and community-based services [14]. The current health
sector five year Programme of Work states a commitment
to promoting mental health [15]. In addition to such policy initiatives, there are increasing numbers of NGOs
working in mental health, and a large research programme consortium, the Mental Health and Poverty
Project (MHaPP) is conducting research on mental health
and poverty within four African countries including
Ghana [16]. This year also saw the relaunch of the Ghana
Mental Health Association, drawing together interested
parties in supporting mental health in the country. In recognition of the burden of mental disorders in Ghana and
the relative paucity of financial and human resources, as
well as its readiness for reform, Ghana is one of the countries which has been identified by the WHO initiative
Mental Health Gap Action Programme (mhGAP) to received
intensified support to scale up treatment for mental, neurological and substance use disorders [17]. As a relatively
stable democracy with a history of psychiatric innovation
and a growing advocacy movement for mental health
within both the health care sector and civil society, Ghana
is facing a unique opportunity to pioneer improved mental health care in the West African region.
Methods
Fieldwork setting
The study centres around a rural town, Kintampo, in
Brong Ahafo, in the central belt of Ghana. Kintampo
forms a transit zone between north and south, and is
Page 3 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
home to many migrant communities now settled in the
town. Kintampo also marks the boundary between two
administrative districts, North and South Kintampo. The
total population of these two districts is about 190,000,
the majority of which live in rural areas. Some of these
rural communities are strung along the main north-south
road, many others are located at some distance along
unpaved feeder roads. Farming is the major occupation
for about seventy per cent of the population in the districts. The most widely spoken language in the district is
Twi, which is spoken by the Akan, the largest ethnic group
in the region as well as in Ghana as a whole, and adopted
by many others as a lingua franca. Other widely used languages in the district include Hausa and English, which is
the official language for government bodies such as education and health services. Over 60% of the population
are Christian, nearly 30% Muslim, and around 8% follow
the traditional religion, though the use of traditional
shrines is more widespread than this figure would suggest.
There are three major sources of help for families in Kintampo North and South districts who have a relative with
mental illness, including biomedical healthcare, 'traditional healing' performed by fetish priests (Twi: akmfo),
and 'faith healing' from Christian pastors or Muslim mallams. Ghana Health Service is the main provider of biomedical care for mental illness, however treatment for
mental disorders seldom penetrates to the community
level. Until 2008 there were no mental health professionals throughout the two Kintampo districts. A Community
Psychiatric Nurse (CPN) has now been posted to Kintampo. In theory she provides a service to the town and
surrounding communities, but since she is provided with
no means of transport she is limited in her capacity to
conduct home visits on a regular basis, particularly to
more distant settlements. Treatment for mental illness at
the community level is largely through the provision of
psychotropic drugs which are available from the district
hospital at Kintampo and from the CPN. Clinics located
in rural communities (sub-districts) are not equipped to
treat mental illness. Inpatient and outpatient psychiatric
care is available in Sunyani, the regional capital, where
there is a psychiatric unit within the regional hospital.
However the three state psychiatric hospitals provide the
major source of inpatient treatment. These are all located
in the south of Ghana, a day's journey from Kintampo
(see figure 1).
By contrast, informal treatment providers are many and
varied, their numbers easily exceeding psychiatric services.
Most communities have an kmfo, a traditional healer or
fetish priest, who under the instruction of the abosom or
'small gods', treats mental illness through the use of
herbal medicines and ritual such as animal sacrifice. Also
popular as sources of healing for mental illness are 'prayer
http://www.globalizationandhealth.com/content/5/1/13
camps' established by Christian pastors who provide healing through prayer, fasting and deliverance from evil spirits. One pastor in Kintampo town is well-known in the
area for his power in healing those who are mentally ill,
and hundreds if not thousands of pastors offer similar
services throughout the country. A shrine in a small rural
community in Kintampo South district is also famed for
healing madness and is visited by people from as far afield
as the Ashanti region and sometimes beyond. Treatment
at prayer camps and shrines often involves a lengthy stay
of several months; sometimes up to a year or even more.
Relatives are usually expected to stay with the patient at
the prayer camps and shrines to provide day-to-day care.
Most frequently this is the mother, but sometimes the
father, sister or another relative takes this role.
Research design
Despite longstanding calls for the contribution of anthropology to explore the influence of culture on the experience and outcome of mental illness [18-20], there are few
detailed ethnographic studies of people living with mental illness in low-income countries. Many studies provide
little detail about the socio-cultural world in which people live, and the ways in which people with mental illness
are treated by their families, friends or the general population [18,19,21,22]. This research draws on the methods
of transcultural psychiatry which views mental illness as a
function of 'the unique experience of being a member of
a particular society: a society with its own characteristic
web of economic constraints, social relations and beliefs'
[23]. Utilising anthropological methods including participant observation, conversation and semi-structured
interviews with people with mental illness, their families,
healers, health professionals and community members
within Kintampo town and the surrounding villages, the
study aimed to discover the particularities of responses to
severe mental illness as embedded within the experience
of living in a rural West African community.
Research subjects
Participants were recruited through purposive sampling at
shrines, churches, prayer camps and family homes. Initially the researchers identified one shrine and two prayer
camps within the Kintampo districts who frequently
treated people with mental illness. The shrine regularly
had 8-10 people with mental illness staying in the compound. However the two prayer camps were relatively
small without a frequent turnover of patients, so a larger
prayer camp was identified in Techiman, a market town
thirty minutes from Kintampo, where there were greater
numbers of people with mental illness. All of these healing centres took patients from across the country, though
predominantly from Brong Ahafo and Ashanti regions.
Permission was sought from the pastor or kmfo to
approach potential participants visiting the shrine/
Page 4 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
http://www.globalizationandhealth.com/content/5/1/13
social functioning. The majority of those studied have
been ill for periods of at least 5 years, some for much
longer than this. Many traced the onset of their illness to
adolescence or early adulthood.
Kintampo
Sunyani
Kumasi
Greater Accra
Cape Coast
Figure
Map
by
participants
of Ghana
1
showing location of psychiatric facilities used
Map of Ghana showing location of psychiatric facilities used by participants.
church. Other participants were recruited from the database of an earlier epidemiological study of psychosis
http://www.iop.kcl.ac.uk/international/?project_id=54,
patients attending the CPN clinic, and through contacts in
the community (see Table 1).
The focus of the study is on those who in Twi would be
described as bdamfo, or a mad person. This behaviour is
identified by local informants with forms of 'wild' and
anti-social behaviour and is closest to what in psychiatric
terms would be labelled psychosis. Frequently described
behaviours include talking to oneself, talking in a disordered way (kasa basabasa), acting aggressively (gidigidi),
and dressing in dirty clothing. The study focuses on those
with more longstanding forms of mental illness which
involve severe disruption of perception, thought, and
Fieldwork
Anthropological fieldwork requires prolonged immersion
in the community under study and participation in everyday life, typically for a period of at least one year, in order
for the researcher to become familiar with local practices
and to minimise the reactivity of informants [24]. Fieldwork took place between October 2007 and December
2008 following a pilot study in June - July 2006. The principal researcher (UMR) lived within Kintampo during the
period of fieldwork, and spent time informally with people living in the Kintampo districts, observing practices
such child-rearing, food preparation, agricultural practices, social relationships and other daily routines. The
fieldwork assistant (SN) was trained in ethnographic
methods, including participant observation and semistructured interviewing. He accompanied the principal
researcher on visits to field sites, and provided assistance
with interpretation, conducting interviews and focus
groups, and arranging entry to the field. The assistant also
functioned as an 'expert informant' during participant
observation, to assist with the explanation of practices
observed, as well as with interpretation. The research consisted of three main approaches: detailed case studies of
people with mental illness, in-depth observation of treatment and healing practices for mental illness, and gathering contextual information relevant to mental illness (see
Appendix 1).
Alongside interviews to elicit verbal accounts, an important part of the research involved spending time with people with mental illness and their families observing their
everyday life and their integration and participation
within the community, including the attitudes of others
towards them. Regular visits were undertaken to the
homes of families who had a relative with mental illness,
to the shrine, and to the three churches treating people
with mental illness. Fieldnotes were written by the
researcher and the assistant to record observations and
conversations following each visit.
During the course of the research over 40 homes were visited in addition to the shrine and prayer camps, and a
total of 67 participants were interviewed including 25
patients, 31 carers, 3 traditional healers, 4 pastors, 1 mallam and 3 imams (see Table 2). Three interviews were in
English, the rest in Twi. Wherever possible we interviewed
the person with mental illness, however some were too
unwell to provide consent or to participate in the interview, in which case we interviewed the main carer, usually
the mother, father or sibling. In eight of the interviews the
carer and the person with mental illness were interviewed
Page 5 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
http://www.globalizationandhealth.com/content/5/1/13
together. This was due to the fact that these patients could
not remember significant details of the time when they
were sick, or suffered from deficits in communication or
cognition which made it difficult to obtain a coherent
interview alone. To obtain contextual information relevant to mental health 7 focus group discussions were held
with a total of 47 participants including registered mental
nurses, young people, Muslims, cannabis users, church
members and parents (see Table 3). Five FGDs were conducted in Twi; two in English. Interviews were semi-structured. For those with mental illness and their family
members questions focused on the history of the person's
illness, the symptoms and course of the illness, possible
causes, the impact of the illness on the individual and the
family in terms of day-to-day life and social roles, sources
of treatment employed, and the experience of such treatment, including its perceived efficacy. For healers interview questions focused on the healers' view of mental
illness, including possible causes, the methods of treatment provided and the ideology/theology on which they
were based, the efficacy of the treatment and the reasons
for this, and views of other forms of treatment and possible collaboration or interaction.
Data analysis
Interviews and focus groups were digitally recorded with
the permission of the informants. Five assistants bi-lingual in Twi and English were recruited and trained. They
transcribed the interviews and focus groups into Twi and
then translated into English. All potentially identifying
details were removed in the transcripts. Analysis utilised a
grounded theory approach in which hypotheses were generated through close examination of the data [24]. Transcripts and fieldnotes were read and recurring themes and
differences noted. The multiple methods used allowed for
some triangulation of the data.
Ethics
Ethical approval for the study was granted by University
College London and Kintampo Health Research Centre
(KHRC). On introduction all participants in interviews
and focus groups were provided with a written information sheet and consent form which was translated into
Twi. As many participants were unable to read Twi the
forms were read to the participants and a verbal explanation of the research aims and methods provided. Questions were invited from participants. Participants were
asked to sign consent forms, or if illiterate to provide
thumb prints in the presence of a witness. Where possible
the researchers aimed to interview the person with mental
illness and the main carer. However if the person with
mental illness was considered too unwell to provide
informed consent, he or she was not interviewed.
It is not feasible nor appropriate to obtain written consent
from all persons who may be involved in observation, for
example a church congregation. The researcher sought the
permission of those in authority at proposed sites, such as
the pastor or traditional healer, before commencing
observation and participation, and ensured that all persons who were involved in periods of observation were
informed of the nature of the research.
Of particular concern in this study were occasions when
the researchers encountered people who were being
treated within the shrine and prayer camps and presented
with severe and distressing symptoms. Where it was
judged by the principal researcher (who has several years
experience as a clinician in mental health services in the
UK) that the person may benefit from psychiatric treatment, the researchers advised the person and their family
of the availability of medical treatment for such illnesses
and the potential benefits. Assistance was provided to
access health services if this was the wish of the family and
the patient. Where a person was considered to be at imminent risk of a serious deterioration in physical or mental
health due to the methods employed by healers the
researcher informed the local CPN and senior researchers
and medical staff at Kintampo Health Research Centre. In
some cases where people with mental illness were
chained, treatment with psychotropic drugs appeared to
improve the mental health of the patient sufficiently for
the family to release the person.
Results
The limits of family care
Almost all those with mental illness encountered in this
research had been chained, either at home, or within healing centres. The most common form of restraint was metal
Table 1: Sampling of cases
Table 2: Interview participants
Source
n=
n=
Epidemiological study of psychosis
Shrine
Prayer camp 1
Prayer camp 2
CPN
Word of mouth
10
9
3
6
4
6
People with mental illness
Carers
Pastors
Traditional healers
Imams/mallams
25
31
4
3
4
TOTAL
38
TOTAL
67
Page 6 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
http://www.globalizationandhealth.com/content/5/1/13
Table 3: Focus group participants
n=
Church members
Muslims (men)
Muslims (women)
Young people
Cannabis smokers
Parents
Registered mental nurses
8
7
7
8
5
7
5
TOTAL
47
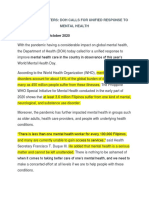
shackles which enclosed the ankles and were attached to a
tree or post (see figure 2). Occasionally people with mental illness were chained to logs.
Caring for a relative with mental illness placed enormous
financial and emotional strain on families, many of
whom were already living with limited resources. Carers
described struggling to manage agitated and aggressive
behaviour. Some reported that a son or daughter had
made threats of violence. One woman for example, had
been chained after threatening her grandmother with a
knife. Another man was chained to a log to prevent him
from preaching loudly during the night and attempting to
stop speeding traffic. In a few cases, some informants
reported being injured by their relative, such as one
mother whose daughter had thrown a piece of metal at
her which had cut her shin very deeply. For some informants, such behaviour led to the family chaining their relative in order to protect themselves.
Outside of the extended family and neighbours, there are
few avenues of support for those in Kintampo districts
attempting to care for a relative with mental illness. Agitated or aggressive behaviour often persuades the family
to seek help at shrines, churches or hospitals, since they
are no longer able to manage their relative at home. The
churches and shrines present the most obvious and accessible resources to assist in restraint and management,
compared to the long and expensive journey to the psychiatric hospitals on the coast, although almost all of
those interviewed had also sought psychiatric treatment
from the hospitals at some point during the course of the
illness. However, given the poor quality of care within the
psychiatric hospitals, the limited efficacy of psychotropic
medication for some informants, as well as unpleasant
side effects, many families saw little evidence of better
alternatives within biomedical treatment. This father of a
young man at the shrine, describes how he had tried both
biomedical and Christian treatment to no effect:
When the illness first occurred I took him to Ankaful [psychiatric hospital] for his brain to be examined, [...] They didn't
explain anything, and prescribed some medicine to give him.
They told us that when the medicine was finished we should go
to Sunyani. So when the medicine was finished, we went back
for more. Yet still, the illness was getting worse, so we went to
a prayer camp.
Interview with father of Kwasi, shrine, 18th June 2008
Spiritual perspectives on mental illness reinforce the popularity of the shrines and churches, since, unlike the hospitals, they address factors such as evil spirits, sorcery and
witchcraft, which are commonly seen to have caused mental illness.
With no ambulance service or medical staff available to
provide an escort, families faced a challenging task bringing disturbed and agitated relatives to places of treatment,
particularly if using public transport, for most the only
affordable means. One relative described how her brother
had to be restrained by seven men in order to bring him
to the shrine for treatment. This family paid the police
who used their handcuffs to restrain the man and bring
him to the shrine in a car.
Chaining of patients is generally conducted with the cooperation of the families who bring their relatives to healing centres. Indeed, several family members reported purchasing the shackles used to restrain their relative. At least
four families visited had also resorted to chaining their
mentally ill relative at home. Carers interviewed at the
shrine and churches were generally accepting of the need
to chain their relative if he or she was 'aggressive', 'roaming around', disruptive or using cannabis. Being 'disturbing' (gidigidi), and 'roaming' (kyinkyin), were common
reasons for the use of chains. The father of Kwasi viewed
the use of chains as important to control his son when he
became loud, hyper-talkative and disruptive, behaviour
which we had witnessed on our visits:
He was mostly chained to a tree. He was released whenever he
calmed down. That is how I saw it....When the sickness came,
he made a noise and they chained him to a tree.
Interview with father of Kwasi, shrine, 18th June 2008
Some parents also seemed haunted by a fear of their child
becoming vagrant, a common fate for those with mental
illness who often seemed compelled to wander far from
home. Akua was living in a prayer camp and had had a
severe mental illness for 10 years. She and her mother provide a typical description of this restlessness that could
lead to people with mental illness wandering into the
bush:
Page 7 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
http://www.globalizationandhealth.com/content/5/1/13
monly associated with dangerousness. The mad are
unpredictable, irrational and potentially violent, as in this
young man's description of a woman who had lived in his
compound and become mentally ill:
...it comes and goes. But when it comes and she sees... she sees
you, she can just pick anything she see on the floor and throw
it on you, and throw it to hit you, maybe to wound you or to kill
you. She'll be sitting down, talking by heart, insulting people,
don't you see? Then laughing....doing all sorts of things.
FGD with young people, 30th April 2008 in English
Figurein2 use in a prayer camp
Chains
Chains in use in a prayer camp.
Akua: I will be standing there talking with someone, and if I go
out I could get lost. And if I get lost, I don't know where I am
going. If someone calls me...
Mother:If it comes likes that she can't stay at home, it makes
her go walking into the bush, it won't allow her to stay at home.
Interview with Akua and mother, prayer camp, 8th May
2008
Vagrants are a common sight in Kintampo town and at the
roadside, most of whom showed signs of mental illness.
For some the use of chains was a means of preventing this
fate for a son or daughter and of keeping him or her
within the family home. We were told moving stories of
family members who had searched for their son or daughter for months; one man had had to go as far as Niger in
search of his brother. During the course of fieldwork, one
of the cases we had interviewed disappeared from home.
Madness and the loss of social status
However, despite this desire to restrain and contain agitated, restless or potentially violent relatives, it was evident that chaining and other forms of harsh treatment
such as beatings, were also embedded within concepts of
mental illness which were influenced by spiritual and
moral understandings of the person and society. Descriptions of the typical 'madman' provided by informants
portrayed him as dirty, unkempt, anti-social, and beyond
the norms of human behaviour. Madness is also com-
Such behaviour directly contravenes social ideals of personhood, in which taking responsibility for others, such
as parenting children, is valued as the mark of adulthood
[25]. The Ghanaian philosopher, Kwasi Wiredu, claims
that for the Akan, 'a person in the true sense is not just any
human being, but one who has attained the status of a
responsible member of society', that is someone who 'is
able to achieve a reasonable livelihood for himself and
family while making non-trivial contributions to the wellbeing of appropriate members of his extended kinship circles and the wider community' [26]. All of those we met
suffering from chronic mental illness were falling well
outside this ideal since most were unable to work, and
almost all were unmarried and childless. Given this failure
to achieve these markers of adulthood and responsibility,
the status of the mentally ill was in some way analogous
to that of a child.
This loss of social status is captured by the concept of a
'spoiled' human being, which was used by some informants to describe those who had become mentally ill. Akua
told us:
'They say that now I'm spoilt. I'm not a human being anymore.'
Interview with Akua, prayer camp, 8th May 2008
The Twi se, translated here as 'spoilt' is a polysemic word,
used to describe moral corruption, bewitchment or bedevilment, rotten food, something gone bad or wasted. One
of the pastors for example, explained how the devil had
'spoiled' a man through alcohol. A 'spoiled' status, as in
Akua's statement, implies a loss of a person's essential
humanity and carries a moral charge. The implication is
that those with mental illness may be subject to forms of
harsh treatment which would not be permitted to other
categories of person.
Chains as part of treatment
The use of chains and shackles formed a routine part of
treatment in the shrine and churches visited. Every healer
visited during the research, whether a Christian pastor or
Page 8 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
a traditional healer, employed shackles on those with
mental illness. Patients were commonly chained when
they were first admitted to a shrine or prayer camp and
removed once the person became calmer, sometimes after
a few days, or a couple of weeks. In very agitated cases, or
where the person was thought to be likely to run away, the
chains were kept on for months. A common concern for
healers and carers was that young men who had been
smoking cannabis would run away to smoke if they were
not chained. Pastors and traditional healers in the area
argue with some validity that they are providing a vital
service for the management of those with mental disorders and many pleaded for greater recognition of their
contribution. Their struggles to manage agitated and
sometimes aggressive patients, as well as distressed and
despairing relatives, called for resources which few were
able to provide. None of the healers had any form of
accommodation of a standard suitable to forcibly detain
patients. Using shackles therefore enabled healers to
enforce treatment such as herbal medicine, 'fasting' and
praying. In the case of Christian pastors, the chains then
became part of fulfilling their divine mission. One pastor
argued that he could not afford to build accommodation
at his prayer camp, so had no alternative but to use chains
to carry out the work God had called him to:
As for me, it is something God has given me, so if I could take
whoever comes here I would be pleased, but the financial problem. And when the mad people come first it is difficult, so we
have to chain them to be able to pray for them for the evil spirit
to leave them, for them to have their peace. There is no money,
otherwise we wouldn't chain them, and I also don't have a room
to put them in.'
Interview with Prophet Agyei, owner of prayer camp, 23rd
June 2006
The two other pastors running prayer camps similarly
reported using chains to manage violent behaviour and
protect others in the public space:
http://www.globalizationandhealth.com/content/5/1/13
harm somebody. We had it tough before we were able to chain
him.
Interview with Maame Grace, owner of prayer camp, 16th
October 2008
However, shackling is not always a response to violent or
uncontrolled behaviour. Madness was commonly seen by
informants as punishment for transgressions and moral
failings such as breaking of taboos, stealing and adultery.
Attributions for the mental illness of some in this study
included the use of sorcery and witchcraft, possession by
evil spirits, and adultery. Madness is also associated with
smoking cannabis which is strongly morally sanctioned,
representing a form of marginalised and anti-social
behaviour, particularly among young men. In line with
this moral perspective on mental illness, chaining and
beating were used for punishment and discipline as well
as restraint within the prayer camps and shrines. Informants described how people were beaten with sticks, belts
and strips of metal and rubber. At the shrine several
informants described how patients were beaten if they
refused to take the herbal medicine, or as punishment for
running away. Since the status of those with mental illness
was akin to an unsocialised child, beating mirrored common methods employed in the disciplining of children,
such as beatings with sticks, although often to a more brutal degree than would be generally acceptable.
Beatings were also part of treatment to rid the person of
evil spirits which were perceived by both pastors and traditional healers to lie behind much mental illness.
Informants in this study described being beaten to drive
away evil spirits such as mmoatia (small forest-dwelling
spirits which were reported to possess several informants,
causing madness), or to extract a confession of wrongdoing or witchcraft. A mother of a patient at the shrine
described how her daughter had been beaten so severely
at a prayer camp, that she had been left permanently
scarred:
So he comes and we get him to sit down, and we are going to
pray, and you are about to pray for him and he will want to hurt
you. Yes. So sometimes we put chains on their legs so that they
won't hurt anybody. Some they go too 'high', so you have to put
chains on their legs so the person becomes calm and you pray
for him.
There [at a prayer camp] they beat her severely with a belt,
today you can see her back, all over her back. They said she
should say she is a witch, but she is not a witch, and so they beat
her severely with a belt, she had wounds all over her back.
Interview with Pastor Owusu, owner of prayer camp 14th
May 2008
Extracting a confession was viewed by healers as important since if the person failed to confess their wrongdoing, they could not be healed.
At the time they brought him, it was very difficult. He was very
violent. When it happened like that, he got new strength. So we
had to put him in chains because if you leave him, he could
Interview with mother of Yaa, shrine, 25th July 2008
There are people maybe they did something evil, and the evil
they did brought the problem [madness]. There are people who
after prayers they have to confess before the healing will come.
Page 9 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
Interview with Prophet Agyei, 23rd June 2006
Healers argued that it was not people themselves who suffered from beatings, but the rather the bad spirits inside
them. Hence beating was morally framed as part of the
battle against the ultimate spiritual cause of mental illness.
In this view chaining and beating is seen as an essential
part of the healing process. By contrast, the removal of the
shackles serves a symbolic purpose for those who treat
mental illness since it is tangible and dramatic demonstration of the efficacy of healing in effecting the transformation of the person from madness to health; from asociality
to humanity. Two of the pastors interviewed had collected
photographs of men and women who had attended their
prayer camps where they were portrayed in a stereotypical
state of madness, in chains with matted or 'bushy' hair,
their semi-naked bodies partially covered by torn and
dirty clothes. Maame Grace displayed 'before and after'
shots side by side in an album, the 'after' photographs
showing the person neatly dressed in new clothes, their
hair cut or styled, released from chains. These photos echoed the story of the Gadarene madman healed by Jesus,
which was cited by the pastors as a Biblical precedent for
their work with the mentally ill. The photographs were
therefore displayed, not as a shameful record of abuse, but
as a visible demonstration of the efficacy of healing. This
was a view shared by some of the carers and even people
with mental illness, who saw the removal of chains as evidence of improvement.
Voices of dissent
However there were those in Kintampo who disagreed
with the harsh treatment given to people with mental illness by pastors and traditional healers. Some family
members interviewed were unhappy with the use of
chains on their relatives. Some had refused to use the
prayer camps or shrines for this reason or had taken their
relative away from such places. The mother of Alice, who
suffered from a long-standing mental illness, had previously sent her to a shrine where she had been chained. She
explicitly compared the treatment of her daughter to that
of an animal, and claimed her daughter's right by contrast
to be treated as a human being:
Ei! It is worrying. It is very sad. She is not a dog that anybody
can chain like that. If she gets up to go to the toilet you have to
remove the chain so she can go. So the person looking after her
feels very sad. It is something to make you sad.
Interview with mother of Alice, Kintampo, 23rd July 2008
Alice's mother's view is particularly striking when one
considered how she had been treated by her daughter
when she was unwell. Alice had frequently publicly
http://www.globalizationandhealth.com/content/5/1/13
insulted her mother, which the researchers had witnessed.
This had progressed to a physical attack on her mother,
however she had refused to punish her:
When she threw the piece of metal, it hit me here [pointing to
shin]. It cut me down to the bone... [...] Her brother said he
would beat her, but I stopped him. This is because she wasn't in
her own mind. If she was in her own mind, she wouldn't hit me
with a piece of metal like that.
Interview with mother of Alice, Kintampo, 23rd July 2008
Importantly, in contrast to the viewpoint of people like
Prophet Agyei, Alice's mother framed her daughter's
behaviour as not being of her own volition, but rather 'out
of her mind': eny n'adwene, literally 'she did not have her
mind'. This phrase carries not only the connotation of losing control of one's own thoughts and behaviour, but of
not being one's true self.
It was striking how few of those who had been subject to
the use of chains or beating complained of their treatment
at the hands of the pastors and fetish priests. However
some of those who had been chained were clearly very distressed by their treatment and expressed resentment
towards the healer and the relative who had placed them
in chains. It was noticeable that the strongest criticism was
voiced by those who were most unwell. Their complaints
were dismissed by carers and healers as symptomatic of
the rebellious behaviour which was part of their madness
and their lack of insight into their mad condition. On one
visit to Maame Grace's prayer camp for example, a teacher
who was shackled begged me to release her and expressed
her anger towards 'that woman' the pastor, who she said
had called her a witch. Another, Moses, angrily contested
his treatment by his mother who had brought him to the
shrine, and told us about the beatings he had received and
the unpleasant sensations he experienced when taking
high doses of herbal medicine which induced a semi-conscious state, and caused diarrhoea. Another male patient
at the shrine complained of the degradation of sitting in
his own urine whilst in chains and threatened to report
the priest once he was released.
Once they were recovered many of those who had been
chained or otherwise harshly treated, conformed to the
general view that their treatment was justified on the
grounds of their madness. Most informants who had
recovered sufficiently to be interviewed expressed little
resentment towards the healer who had chained them,
viewing it as a necessary part of the process of healing and
perhaps unavoidable given their disturbed behaviour.
Some stated that the chains had 'helped' because it had
made them comply with the treatment or had acted as a
form of 'negative reinforcement':
Page 10 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
When I first came here, I was put in chains because they
thought I would run away. I was in chains for three days and
was given some herbal medicine to take. I don't consider this as
maltreatment but a way to treat me and see to it that I am well.
Interview with Kwabena, shrine, 18th October 2008
Notably some young men had chosen to stay and serve
the pastors who had formerly chained them, training as
pastors themselves and doing other work such as farming,
maintenance and running errands. In turn they too
assisted in the chaining of other patients with mental illness. For some informants the church and the shrine provided important social and material support and a refuge
from stigma in the home community. The pastors, for
example, provided subsistence such as food, clothing and
accommodation in return for farming on their land, offering one option for survival in a region where there are very
high rates of youth unemployment, particularly for young
men.
http://www.globalizationandhealth.com/content/5/1/13
rural and urban areas, leading to financial burden, emotional strain and social stigma. This research also reported
how families had struggled to manage difficult and sometimes violent behaviour by people with mental illness
towards family members, such as beatings and setting
fires. Churches and mosques were reported to be important sources of material help [33]. In countries where
social structure and health care has been devastated by
war, government resources for the treatment and care of
those with mental illness are even more scarce. A recent
Channel 4 documentary shown in the UK, for example,
provided graphic coverage of the use of chains within
Sierra Leone's sole psychiatric hospital (staffed by the
country's only psychiatrist), and within the compounds of
traditional healers. In this film, both the psychiatrist and
healers defended the use of chains as necessary to prevent
their patients running away from treatment [34].
Enhancing mental health care
The challenges of providing mental health care in accordance with international human rights standards as shown
in Kintampo have been noted elsewhere in Africa. Alem
reports the use of ropes and shackles to restrain people
with mental disorders in homes and traditional healing
centres in Ethiopia. He remarks that in Ethiopia the provision of care in 'modern and traditional institutions' is not
in accordance with protection of human rights as defined
by 'western culture', however he argues that given the scarcity of resources for mental health care 'these procedures
have protected many patients from vagrancy, and from
the danger of deterioration which could arise from lack of
treatment.' [27]. In Nigeria, Eaton and Agomoh report
that traditional healers and "prayer houses" employ
herbal remedies, chaining, beating, cutting of the skin,
acid burning or starvation ("fasting") in the treatment of
the mentally ill and 'serve a purpose as a means of containment'. The scarcity and expense of psychiatric services
impedes their use by many. This is coupled with a lack of
knowledge and doubts about the effectiveness of medical
treatment for mental illness which is seen as caused by
'spiritual attack' [28].
The Global Movement for Mental Health has explicitly
linked the scaling up of mental health services with the
protection of the human rights of those with mental disorders, promoting the development of policies and legislation to both enhance the provision of mental health
care, and to protect human rights. The scarcity of accessible and high quality mental health care undoubtedly contributes to the continued popularity of traditional healers
and prayer camps, and to the high attrition from psychotropic treatment. However as this research shows, other
factors such as the belief in spiritual influences on mental
health and a scepticism towards the effectiveness of biomedicine for mental disorders also result in families seeking alternatives to psychiatric treatment. Psychiatric
hospitals are notorious within Ghana as elsewhere in subSaharan Africa for being over-crowded and under-funded.
Quality of care is compromised by the low numbers of
qualified staff, the paucity of on-going staff training, and
a lack of psychosocial treatment and rehabilitation [35].
There are reports of beatings and the use of medication as
punishment [36]. If psychiatric services are to be seen by
people with mental illness and their carers as a viable
alternative or adjunct to other forms of treatment, then
they must not only reach out to rural communities, but
also provide the highest standard of care which promotes
human rights and respects the viewpoint of the person
being treated.
As shown in this study, given the lack of state welfare provision in many African countries, responsibility for the
care of those with severe mental illness lies with the family, leading to a significant carer burden [29-33]. A study
in Nigeria showed that caregiver burden was higher where
the relative demonstrated psychotic symptoms and 'uncooperative behaviour' [32]. As in this research, a study in
Ghana of family responses to mental illness found that
the family provided the main source of support in both
Local struggles and human rights
In this research it was notable that in contrast to international outrage within scientific journals and the media of
Western states, the widespread use of shackles and other
forms of maltreatment towards those with mental illness
in Kintampo and the surrounding communities provoked
remarkably little protest within the communities studied.
Whilst there have been some criticisms of the harsh treatment of people with mental illness by traditional and
Discussion
Page 11 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
faith healers in national newspaper articles, reports
[13,37-39], and NGO campaigns in Ghana, these have
had little impact at the local level. The Commission on
Human Rights and Administrative Justice (CHRAJ) has an
office in Kintampo only a short walk from one of the
churches where chains are routinely employed. CHRAJ is
a national government funded organisation whose mandate is to promote, protect and enforce fundamental
human rights and freedoms through providing mediation, advocacy and legal support. Yet there has been no
move to sanction the practice of chaining and other forms
of maltreatment employed either by individual families
or by healers. In August 2007 officials at the Kintampo
office of CHARJ reported that no one had petitioned them
regarding the human rights of people with mental illness,
hence they had not taken up the case. Local health practitioners were also aware of the practices of local healers
within their district.
From conversations and observation it appeared that families rather than the state were judged to be responsible for
the welfare of their relative if they chose to use such treatment. Yet, it is at the level of state intervention that solutions are most often proposed. In Ghana for example, the
attention of national leaders in psychiatry has focused on
legislation to outlaw practices such as chaining. A new
mental health law has been drafted which overtly adopts
a 'human rights based approach' reflecting current international guidelines as articulated by WHO [40], although
it has not yet been passed. This bill explicitly prohibits
abuse within healing facilities, including traditional healers and 'spiritual mental health facilities' [41]. However
the capacity of this act to effect imminent change in the
treatment of the mentally ill is cautioned by the fact that
within Kintampo districts existing legislation which
should in theory protect the rights of the mentally ill, is
routinely breached with impunity. The Mental Health
Decree (1972), which forms current mental health legislation, does not address the issue of restraint or maltreatment by relatives or healers, however it does provide for
the police to remove to 'a place of safety' any person suspected of suffering from mental illness who 'has been, or
is being, ill-treated, neglected or kept otherwise than
under proper control' [42]. The Constitution of Ghana
which aims to protect the rights of all citizens, states that
no person who is restricted or detained should be subjected to 'cruel, inhuman or degrading treatment or punishment' and 'any other condition that detracts or is likely
to detract from his dignity and worth as a human being.'
(Clause 15(2)) [43].
Leaving aside the question as to whether the chaining of
those with mental illness is perceived by those who
employ it as 'cruel, degrading, or inhuman', or whether it
is rather viewed as an unfortunate necessity, even as mun-
http://www.globalizationandhealth.com/content/5/1/13
dane, the failure of existing legislation to impact on the
treatment of the mentally ill in rural communities such as
Kintampo, raises important questions about the viability
of further legislation to protect people with mental illness
from human rights abuses. National legislation may echo
the best of the international human rights discourse with
its language of freedom and rights, however many of
those whom it seeks to protect would struggle to understand it, if they were even aware of its existence. The weakness of much human rights legislation, as has been
cautioned of civic education campaigns in Malawi, is that
'the starting point is not the actual concerns and aspirations of the people, their particular situations in life and
experiences of abuse, but freedom, democracy, and
human rights as universal and abstract values.' [44]
Where, as in Ghana, there is little faith in the efficacy of
state apparatus, and law enforcement agencies are both
over-stretched and corrupt, protecting human rights often
falls to families and healers rather than the state. As
argued by Farmer and Gastineau, 'rights attributed on
paper are of little value when the existing political and
social structures do not afford all individuals the ability to
enjoy these rights, let alone defend them.' [10].
Morality and rights
A further caution concerns the focus on individual rights
within the human rights discourse employed by international agencies such as WHO. The approach to rights
enshrined within much human rights legislation is largely
founded on European concepts of the person as a selfdetermining individual. By contrast, the actions of family
members and healers observed in this study reflect a concern with the safety and moral integrity of the group,
rather than the individual rights of the person with mental
illness. This reflects Ghanaian ideals concerning the
sociality of human beings and relationships of reciprocity
and responsibility, and the sanctioning of overt individualism. Within Ghana, as Englund [45] describes for
Malawi, human rights may be viewed as grounded within
a moral rather than legal framework, one which draws on
'traditional' morality as articulated at the shrines, and
increasingly on Christian moral codes. Gyekye writes that
'Within the framework of Akan social and humanistic ethics, what is morally good is that which promotes social
welfare, solidarity, and harmony in human relationships'.
By contrast, moral evil (bone) is 'that which is considered
detrimental to the well-being of humanity and society'
[46]. In this view rights carry responsibilities, and are
earned, rather than innate. This moral approach which
emphasises both rights and responsibilities, suggests the
need to engage with all the players involved in the use of
methods such as chaining to find a way forward. It has
been argued that in contrast to the absolutist division
within human rights discourse between victims and violators, there is a need for 'less self-righteous modes of relat-
Page 12 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
http://www.globalizationandhealth.com/content/5/1/13
ing that are also more attuned to moral complexity:
listening, compromise and the creation of new solidarities
and practices of co-existence based on recognition of an
imperfect shared humanness.' [47]. This approach may
open a way for dialogue which avoids alienating those
perceived within the human rights discourse as 'violators',
and recognizes their sometimes legitimate concerns, for
example for the safety of the community.
MHaPP in Kintampo to promote the human rights of people with mental illness in the district. Initiatives such as
these, which establish a dialogue with local actors, could
begin to address the factors which contribute to the continued use of chaining and other forms of abuse, and
work alongside families and healers to protect and promote the rights, dignity and health of those with mental
illness.
However it should be cautioned that such a moral perspective on rights and responsibilities may also be used to
justify the maltreatment of the mentally ill as this research
has suggested. The morally suspect status of the mentally
ill may be seen to threaten the cohesion and moral integrity of the group, thus they may be excluded from entitlement to the rights otherwise accorded to morally upright
and socialised human beings. Their rights are likely to be
subsumed to the needs of the group thereby sanctioning
the use of whatever means necessary to control behaviour
which threatens this cohesion. As this research shows, to
fail to address the issue of the chaining of the mentally ill
and other practices of restraint, is to ignore the significant
cost for those chained and beaten: socially, physically and
psychologically. Several patients had suffered lasting
physical damage as a result of being chained for long periods, such as muscle wasting and shortening. Many bore
scars on their ankles, evidence of the abrasion caused by
the shackles. Some were resentful of the treatment
received at the hands of their families, or of healers or pastors into whose care they had been entrusted by family
members. In some cases this can lead to a breakdown in
family relationships from which some families never
recover. The ultimate risk surrounding attempts at chaining and restraining those who are agitated or aggressive,
was tragically illustrated during the course of fieldwork. In
May 2008 a young police officer experienced a mental
breakdown whilst in a church in Kintampo, and began to
behave aggressively, smashing objects and shouting. As
yet the facts of the case have not been verified, however it
appears that in the course of attempts to restrain him by
church elders, the man's neck was broken and he died.
Limitations
This study suffers from a number of limitations most of
which are inherent in the anthropological approach with
its focus on 'ethnographies of the particular' [48] and the
use of key informants. Whilst it provides an indepth study
of factors surrounding responses to mental illness within
the communities under study, caution should be exercised in generalising these findings elsewhere since the
sample size is small and particular personal, historical,
social and cultural factors will vary. Ideally a greater
engagement between such qualitative anthropological
studies and quantitative research utilising standardised
instruments along the lines suggested by De Jong and Van
Ommeren for cross-cultural epidemiology [49] could provide a means of counterbalancing the limitations of both
methodologies within international mental health
research. Whilst the long period spent in the field may
have helped to minimise the effect of the researchers during participant observation and interviews to some
degree, the presence of both educated Ghanaian researchers and a white European researcher undoubtedly influenced the responses provided in both positive and
negative ways. For example, the informants may have
been able to say things to a 'stranger' that they could not
say to a member of the community, but equally they may
not have been willing to disclose other facts to 'strangers'.
The use of Twi as the lingua franca may have disadvantaged those for whom it was not their first language, and
the process of translation inevitably leads to some loss or
distortion of meaning. We attempted to minimise this
through transcription first into Twi and through explanation of the Twi words used where these were polysemic
and had no direct translation in English.
There are some signs in Kintampo of an uneasiness with
the practice of chaining, and a desire for other alternatives
on the part of those involved in treating the mentally ill.
A few families strongly resisted the use of chains on their
relatives and chose to forgo the treatment offered by spiritual healers where such methods were employed. A pastor whose church routinely chains the mentally ill to trees,
expressed the opinion that such treatment is 'not the best',
and stated his desire for funding so that better facilities for
the confinement of patients could be provided. Since
2008 representatives from CHRAJ, the District Health
Management Team, traditional and faith healers, carers
and people with mental illness are co-operating with the
Conclusion
There remains a gap between the global discourse on
health (one conducted largely in English, the language of
power), which is echoed within the corridors and conference rooms of ministries of health within Ghana and
other low-income countries, and the conversations and
decisions around health care which take place at community level. This research illustrates some of the challenges
faced by families in supporting relatives with mental illness, and the suffering endured by those who are subjected to chaining, beating and other forms of harsh
treatment within healing centres and family homes. As
Page 13 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
this study has shown, many families allow their relatives
to be chained in order to provide treatment which is perceived to be in their best interests, and to control and punish difficult behaviours. Counter-intuitively, the use of
chains can therefore represent an attempt to maintain the
care of severely mentally ill relatives in the absence of avenues of support and at great emotional, social and material cost. Such practices are also rooted within accepted
responses to mental illness within the study area, drawing
on historical, cultural and symbolic meanings, and thus
do not evoke the level of protest that might be expected
within a discourse of human rights. Indeed, the emphasis
on individual human rights employed by international
agencies may fail to engage with local concerns underlying practices of restraint, and the need to provide viable
alternatives which will support both those with mental illness and their families.
In arguing for a 'scaling up' of mental health care The Global Movement for Mental Health and WHO should be wary
of a 'one size fits all' approach that may fail to recognise
local resources and concepts of mental health and illness
which sometimes sit uneasily with biomedical
approaches to psychiatric treatment. As argued by Alem
for Ethiopia [27], mental health care predicated solely on
Western models is unlikely to be realistic in the context of
the limited resources available in low-income countries of
sub-Saharan Africa, nor may it be the best response to the
particular needs of rural communities. Research in Malawi
suggests that greater knowledge of biomedical models of
mental illness may not necessarily reduce carer burden
[50]. However providing an outreach service for people
with schizophrenia in rural India which provided psychosocial support and advice, alongside psychotropic medication, was shown to reduce symptoms, disability and
family burden [51]. In rural Nigeria other approaches to
facilitating access to mental health services and working
with families include involving family members in providing treatment and combating stigma [52], and the
training of village health workers [28]. Given the important role of families and informal healers in Ghana in providing care and managing the challenging behaviours
sometimes displayed by those with serious mental illness,
mental health services need to consider how best to
strengthen family resources and engage with local healers
to present realistic alternatives to chaining. There is also a
need to confront deep-rooted historical and cultural practices which inform responses to mental illness at the level
of families and the broader society. This is evidently more
difficult, since it involves the changing of attitudes. Legislation alone is unlikely to alter practices used for the
restraint of those with mental illness, unless it is coupled
with a commitment to funding mental health services.
These services must be flexible enough to reach out to
rural communities if they are to be accessible to families
http://www.globalizationandhealth.com/content/5/1/13
with few material or financial resources to access treatment at more distant health care facilities. They must also
be creative enough to overcome the limitations of a strict
biomedical psychiatry and find ways of working with
local families and healers to improve the care of those
with mental illness and relieve something of the burden
felt by many carers.
Legislation to protect the human rights of people with
mental illness is undoubtedly a vital tool to regulate
abuses within both government and private treatment
facilities. However such legislation is likely to prove
harder to implement within small rural communities
which are distant from the reach of the state, and will be
beyond the means of many to exploit for their protection.
Ultimately engaging with local actors as they struggle to
live with mental illness and search for a cure, may promise
more in terms of changing responses to mental illness
than creating legal sanctions which are unlikely to provide
immediate benefits in the short term.
Appendix 1: Outline of methods
Case studies
Visits to case families at home and/or healing facility
Participant observation of everyday life e.g. work, family
interactions, social activities
Observation and conversation with people with mental
illness and family/friends
Semi-structured interviews with people with mental illness and family members
Healing resources for mental illness
Participant observation of healing rituals and practices at
shrines and prayer camps
Visits and observation at health facilities (psychiatric
hospitals, CPN clinics, general hospitals, rural clinics) and
conversation with health workers
Visits to mental health NGOs
Semi-structured interviews with healers, pastors and
people attending healing facilities
Concepts of and attitudes towards mental illness
Content analysis of media representations of mental illness e.g. newspaper articles, TV, films
Exploration of popular knowledge of mental illness as
revealed in proverbs, folk tales, symbolic representations
etc.
Page 14 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
http://www.globalizationandhealth.com/content/5/1/13
Focus groups with nurses, church members, Muslims,
young people, parents etc.
16.
Competing interests
17.
The authors declare that they have no competing interests.
Authors' contributions
UMR conceived of the study, and developed its design.
She participated in all aspects of the research and prepared
the draft of the manuscript. SN completed the interviews
and focus group discussions, participated in fieldwork,
and helped develop the research questions. SN and EA
read the manuscript and provided additional comments.
All authors edited and approved the final manuscript.
18.
19.
20.
21.
Acknowledgements
We gratefully acknowledge the support of Kintampo Health Research Centre in conducting this study, in particular Dr Victor Doku, Dr Seth Owusu
Agyei, and the mental health research team. We also thank Ms Mary
Lamptey, CPN Kintampo. The study was funded by the Economic and Social
Research Council, UK in collaboration with Kintampo Health Research
Centre who provided logistical support.
22.
References
26.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
WHO: Global Burden of Disease 2004 Update. Geneva: World
Health Organization; 2008.
Gureje O, Lasebikan V: Use of mental health services in a developing country. Soc Psychiatry Psychiatr Epidemiol 2006, 41:44-49.
WHO: Mental Health Atlas 2005 [http://www.who.int/mental_health/
evidence/mhatlas05/en/index.html]. Geneva. World Health Organization
WHO: The World Health Report 2001: Mental Health: New Understanding, New Hope 2001 [http://www.who.int/whr/2001/en/]. Geneva.
World Health Organization
Lancet Global Mental Health Group: Scale up services for mental
disorders: a call for action. The Lancet 2007, 370:1241-1252.
United Nations: Principles for the protection of persons with mental illness
and the improvement of mental health care 1991 [http://www.un.org/
documents/ga/res/46/a46r119.htm]. Office of the High Commissioner
for Human Rights, Resolution 46/119
Maingay S, Thornicroft G, Huxley P, Jenkins R, Szmukler G: Mental
health and human rights: the MI Principles-turning rhetoric
into action. International Review of Psychiatry 2002, 14:19-25.
United Nations: Convention on the Rights of Persons with Disabilities and
Optional Protocol 2006 [http://www.un.org/esa/socdev/enable/rights/
convtexte.htm].
WHO: Mental Health Legislation and Human Rights. In Mental Health Policy and Service Guidance Package Geneva: World Health
Organization; 2003.
Farmer P, Gastineau N: Rethinking health and human rights:
time for a paradigm shift. J Law Med Ethics 2002, 30:655-666.
Read UM, Doku VCK, De-Graft Aikins A: Schizophrenia and psychosis in West Africa from the colonial era to the present. In
Culture, Mental Illness and Psychiatric Practice in Africa Edited by:
Akyeampong E, Hill A, Kleinman A. Cambridge: Indiana University
Press in press.
Forster EB: The Theory and Practice of Psychiatry in Ghana.
Am J Psychother 1962, 16:7-51.
Commonwealth Human Rights Initiative Africa: Human Rights Violations in Prayer Camps and Access to Mental Health in Ghana Accra: CHRI;
2008.
WHO: Ghana Country Summary. Mental Health Improvement for Nations
Development
(MIND)
Geneva
2007
[http://www.who.int/
mental_health/policy/country/countrysummary/en/index.html].
Department of Mental Health and Substance Abuse
Ministry of Health Ghana: Creating Wealth Through Health: The Health
Sector Programme of Work 2007-2011 [http://www.moh-ghana.org/
moh/docs/programs_of_work/pows/5YPoW(2007-2011).pdf].
23.
24.
25.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
Flisher AJ, Lund C, Funk M, Banda M, Bhana A, Doku V, Drew N, Kigozi FN, Knapp M, Omar M, et al.: Mental health policy development and implementation in four African countries. Journal of
Health Psychology 2007, 12:505-516.
WHO: Mental Health Gap Global Action Programme: Scaling Up Care for
Mental, Neurological and Substance Use Disorders 2008 [http://
www.who.int/mental_health/mhgap/en/index.html]. Geneva. World
Health Organization
Craig TJ, Siegel C, Hopper K, Lin S, Sartorius N: Outcome in schizophrenia and related disorders compared between developing and developed countries: a recursive partitioning reanalysis of the WHO DOSMD data. Br J Psychiatry 1997,
170:229-233.
Edgerton RB, Cohen A: Culture and schizophrenia: the
DOSMD challenge. Br J Psychiatry 1994, 164:222-231.
Hopper K: Interrogating the meaning of "culture" in the
WHO international studies of schizophrenia. In Schizophrenia,
Culture and Subjectivity: the Edge of Experience Edited by: Jenkins JH,
Barrett RJ. Cambridge: Cambridge University Press; 2004:62-86.
Harrison G, Hopper K, Craig T, Laska E, Siegel C, Wanderling J, Dube
K, Ganev K: Recovery from psychotic illness: a 15- and 25-year
international follow-up study. Br J Psychiatry 2001, 178:506-517.
Patel V, Cohen A, Rangaswamy T, Gureje O: Is the outcome of
schizophrenia really better in developing countries? Revista
Brasileira de Psiquiatria 2006, 28:149-152.
Littlewood R: The Butterfly and the Serpent: Essays in Psychiatry, Race
and Religion London; New York: Free Association Books; 1998.
Bernard HR: Research Methods in Anthropology: Qualitative and Quantitative Approaches 4th edition. Lanham: Altamira Press; 2006.
Miescher SF: Making Men in Ghana Bloomington; Indianapolis: Indiana
University Press; 2005.
Wiredu K: Cultural Universals and Particulars: An African Perspective
Bloomington: Indiana University Press; 1996.
Alem A: Human rights and psychiatric care in Africa with particular reference to the Ethiopian situation. Acta Psychiatr
Scand 2000, 101:93-96.
Eaton J, Agomoh AO: Developing mental health services in
Nigeria: the impact of a community-based mental health
awareness programme. Soc Psychiatry Psychiatr Epidemiol 2008,
43:552-558.
Shibre T, Kebede D, Alem A, Negash A: Schizophrenia: illness
impact on family members in a traditional society- rural
Ethiopia. Soc Psychiatry Psychiatr Epidemiol 2003, 38:27-34.
Ukpong DI: Demographic factors and clinical correlates of
burden and distress in relatives of service users experiencing
schizophrenia: A study from south-western Nigeria. International Journal of Mental Health Nursing 2006, 15:54-49.
Martyns-Yellowe I: The burden of schizophrenia on the family:
a study from Nigeria. Br J Psychiatry 1992, 161:779-782.
Ohaeri JU: Caregiver burden and psychotic patients' perception of social support in a Nigerian setting. Soc Psychiatry Psychiatr Epidemiol 2001, 36:86-93.
Quinn N: Beliefs and Community Responses to Mental Illness
in Ghana: The Experiences of Family Carers. Int J Soc Psychiatry
2007, 53:175-188.
Sierra Leone: Insanity of War. Unreported World, Channel 4 2009.
Doku V, Ofori-Atta AL, Akpalu B, Read U, Osei A, Ae-Ngbise K,
Awenva D, Lund C, Flisher AJ, Petersen I, et al.: A Situation Analysis of
Mental Health Policy Development and Implementation in Ghana 2008
[http://workhorse.pry.uct.ac.za:8080/MHAPP]. Mental Health and
Poverty Project
Roberts H: A way forward for mental health care in Ghana?
The Lancet 2001, 357:1859.
Selby H: Mental Illness, Prayer Camps And Society: A Factor
of Human Rights Abuse. The Ghanaian Chronicle. Accra 2008.
Asiedu W, Kwei R: Patients chained at prayer camp. The Mirror.
Accra 2004.
Vinorkor M-A: Move to Protect Mental Patients. The Daily
Graphic. Accra 2004.
WHO: WHO Resource Book on Mental Health, Human Rights and Legislation Geneva. World Health Organization; 2005.
Government of Ghana: Mental Health Bill. Ghana 2006.
National Redemption Council Ghana: Mental Health Decree
NRCD 30. Ghana 1972.
Government of Ghana: The Constitution of the Republic of Ghana 1992
[http://www.ghana.gov.gh/ghana/constitution_republic_ghana.jsp].
Page 15 of 16
(page number not for citation purposes)
Globalization and Health 2009, 5:13
44.
45.
46.
47.
48.
49.
50.
51.
52.
http://www.globalizationandhealth.com/content/5/1/13
Englund H: Prisoners of Freedom: Human Rights and the African Poor Berkeley; Los Angeles; London: University of California Press; 2006.
Englund H: The dead hand of human rights: contrasting Christianities in post-transition Malawi. The Journal of Modern African
Studies 2000, 38:579-603.
Gyekye K: An Essay on African Philosophical Thought: The Akan Conceptual Scheme Cambridge: Cambridge University Press; 1987.
Turner T, Graham LR, Fluehr-Lobban C, Cowan JK: Do anthropologists have an ethical obligation to promote human rights?
An open exchange. In Human Rights: An Anthropological Reader
Edited by: Goodale M. Chichester: Wiley-Blackwell; Blackwell Readers in Anthropology; 2009:198-205.
Abu-Lughod L: Writing Against Culture. In Recapturing Anthropology: Working in the Present Edited by: Fox RG. Santa Fe: School of
American Research Press; 1991.
de Jong JTVM, Van Ommeren M: Toward a Culture-informed
Epidemiology: Combining Qualitative and Quantitative
Research in Transcultural Contexts. Transcultural Psychiatry
2002, 39:422-433.
Sefasi A, Crumlish N, Samalani P, Kinsella A, O'Callaghan E, Chilale H:
A little knowledge: caregiver burden in schizophrenia in
Malawi. Soc Psychiatry Psychiatr Epidemiol 2008, 43:160-164.
Murthy RS, Kumar KVK, Chisholm D, Thomas T, Sekar K, Chandrashekar CR: Community outreach for untreated schizophrenia in rural India: a follow-up study of symptoms,
disability, family burden and costs.
Psychol Med 2005,
35:341-351.
Patkai I: Relatives help abolish physical restraints in Northern
Nigeria: The role of the family in inpatient psychiatric care.
Global Forum for Community Mental Health [http://www.gfcmh.com/
?page_id=118]. Accessed 6th May; 2009
Publish with Bio Med Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours you keep the copyright
BioMedcentral
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
Page 16 of 16
(page number not for citation purposes)
Você também pode gostar
- Mental Health Worldwide: Culture, Globalization and DevelopmentNo EverandMental Health Worldwide: Culture, Globalization and DevelopmentAinda não há avaliações
- Primary Care Mental Health in Older People: A Global PerspectiveNo EverandPrimary Care Mental Health in Older People: A Global PerspectiveCarlos Augusto de Mendonça LimaAinda não há avaliações
- Mental Heath AFRDocumento16 páginasMental Heath AFRthursday8893Ainda não há avaliações
- Mental Health Gap - South AfricaDocumento15 páginasMental Health Gap - South AfricaMunyai KHAKHUAinda não há avaliações
- CENA C2.editedDocumento21 páginasCENA C2.editedEllen Gonzalvo-CabutihanAinda não há avaliações
- Guideline MinimunDocumento14 páginasGuideline MinimunsofinoyaAinda não há avaliações
- Position PaperDocumento14 páginasPosition Paperantonette gammaru100% (1)
- Global Burden of Mental Disorders and The Need For A Comprehensive, Coordinated Response From Health and Social Sectors at The Country LevelDocumento6 páginasGlobal Burden of Mental Disorders and The Need For A Comprehensive, Coordinated Response From Health and Social Sectors at The Country Levelmohsen ghaffariAinda não há avaliações
- Dementia: A Public Health PriorityDocumento112 páginasDementia: A Public Health PriorityEmanuel SantanaAinda não há avaliações
- Scaling-Up Mental Health ServicesDocumento12 páginasScaling-Up Mental Health ServicesPierre LaPaditeAinda não há avaliações
- Mental Health ServicesDocumento3 páginasMental Health ServicesAntonette NangAinda não há avaliações
- PP Who AvikaDocumento3 páginasPP Who Avikapriyagaur27Ainda não há avaliações
- Mental Illness PDFDocumento13 páginasMental Illness PDFRaquel De LeonAinda não há avaliações
- Mental Health StudyDocumento4 páginasMental Health StudyKrishna SapkotaAinda não há avaliações
- Zamora CHN ResearchDocumento9 páginasZamora CHN ResearchHazelGatuslaoZamoraAinda não há avaliações
- The World Federation For Mental Health Africa InitiativeDocumento11 páginasThe World Federation For Mental Health Africa InitiativeJames ChaulukaAinda não há avaliações
- Bartlett, Hugh H. - Madness, Medicine, and Witchcraft in Bududa, Uganda (2017)Documento39 páginasBartlett, Hugh H. - Madness, Medicine, and Witchcraft in Bududa, Uganda (2017)Pedro SoaresAinda não há avaliações
- Beyond Evidence The Moral Case For International MDocumento5 páginasBeyond Evidence The Moral Case For International MChinaza AjuonumaAinda não há avaliações
- Barriers To Improvement of Mental Health Services in Low - Middle Income CountriesDocumento11 páginasBarriers To Improvement of Mental Health Services in Low - Middle Income CountriesmoyrgosAinda não há avaliações
- WHO Netherlands Fajriyatul KamalDocumento2 páginasWHO Netherlands Fajriyatul KamalFajriyatul KamalAinda não há avaliações
- Overview of Mental IllnessDocumento15 páginasOverview of Mental IllnessbeibhydAinda não há avaliações
- Mental Health Awareness 2Documento5 páginasMental Health Awareness 2Kuro AkiAinda não há avaliações
- Surgeon General Mental Health Report - 1999 - DCF PDFDocumento494 páginasSurgeon General Mental Health Report - 1999 - DCF PDFatjoeross100% (2)
- World Mental Health Day - 2022Documento17 páginasWorld Mental Health Day - 2022TesitaAinda não há avaliações
- Researcharticle Open Access: Sharon Kleintjes, Crick Lund and Leslie SwartzDocumento10 páginasResearcharticle Open Access: Sharon Kleintjes, Crick Lund and Leslie SwartzLocklinaAinda não há avaliações
- Global Burden of Mental Disorders and The Need For A Comprehensive, Coordinated Response From Health and Social Sectors at The Country LevelDocumento7 páginasGlobal Burden of Mental Disorders and The Need For A Comprehensive, Coordinated Response From Health and Social Sectors at The Country LevelstatuhominisAinda não há avaliações
- Mental Health Class NotesDocumento3 páginasMental Health Class Notessuz100% (4)
- Letter To The Global Fund On IDU Strategy English #PF2011Documento9 páginasLetter To The Global Fund On IDU Strategy English #PF2011AB-Ainda não há avaliações
- Primary Health Care: Mental Health in PakistanDocumento6 páginasPrimary Health Care: Mental Health in PakistanQaiser ZamanAinda não há avaliações
- Moron-Nozaleda Et Al (2011) - Integrating Mental Health Into Primary Care In.11Documento11 páginasMoron-Nozaleda Et Al (2011) - Integrating Mental Health Into Primary Care In.11Alberto Fernandez LiriaAinda não há avaliações
- Advocacy ProgramsDocumento13 páginasAdvocacy ProgramsDanica Mae Bianito100% (1)
- Attitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyDocumento6 páginasAttitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyAdina OlteanuAinda não há avaliações
- AIDSTAR-One Technical Brief: Human Rights Considerations in Addressing HIV Among Men Who Have Sex With MenDocumento18 páginasAIDSTAR-One Technical Brief: Human Rights Considerations in Addressing HIV Among Men Who Have Sex With MenAIDSTAROneAinda não há avaliações
- Fourth Report of Committee A: (Draft)Documento31 páginasFourth Report of Committee A: (Draft)BlanksillasAinda não há avaliações
- Chapter IiDocumento14 páginasChapter IiSzia Darene MARTINAinda não há avaliações
- Background 1Documento3 páginasBackground 1Abdulahi SaedAinda não há avaliações
- DES 312 Health in DevelopmentDocumento188 páginasDES 312 Health in DevelopmentPastor-Oshatoba Femi JedidiahAinda não há avaliações
- Community Mental HealthDocumento17 páginasCommunity Mental HealthNicholeAinda não há avaliações
- Complementary and Integrative Health Care Management of Dementia Among The Elderly in CaviteDocumento13 páginasComplementary and Integrative Health Care Management of Dementia Among The Elderly in CaviteperezAinda não há avaliações
- Tatenda Amanda MudinzwaDocumento21 páginasTatenda Amanda MudinzwaTatenda Amanda MudinzwaAinda não há avaliações
- Mental Health ProgramDocumento4 páginasMental Health ProgramMADULI, Marlone G.100% (1)
- 13 CulturalPerspectivesandAttitudestoward PDFDocumento11 páginas13 CulturalPerspectivesandAttitudestoward PDFKabeloAinda não há avaliações
- 13 CulturalPerspectivesandAttitudestoward PDFDocumento11 páginas13 CulturalPerspectivesandAttitudestoward PDFKabeloAinda não há avaliações
- Global Mental Health Action PlanDocumento22 páginasGlobal Mental Health Action PlanJenezon CardenioAinda não há avaliações
- CH11 Control of NCDSDocumento35 páginasCH11 Control of NCDSIrish CacayanAinda não há avaliações
- Problematic Recipe: Alternatives To Public Health Education To Reduce The HIV PandemicDocumento18 páginasProblematic Recipe: Alternatives To Public Health Education To Reduce The HIV PandemicfadligmailAinda não há avaliações
- Position Paper Alemunx - Topic A PDFDocumento6 páginasPosition Paper Alemunx - Topic A PDFSofia TortorellaAinda não há avaliações
- Global Mental HealthDocumento4 páginasGlobal Mental HealthFIRDA NURSANTIAinda não há avaliações
- WHO Dementia A Public Health PriorityDocumento112 páginasWHO Dementia A Public Health PriorityJuliet Corner100% (1)
- CU Week 13 mhGAP (MENTAL HEALTH GLOBAL ACTION PROGRAM)Documento12 páginasCU Week 13 mhGAP (MENTAL HEALTH GLOBAL ACTION PROGRAM)Mizuiro SenpaiAinda não há avaliações
- Global Health Research Paper TopicsDocumento6 páginasGlobal Health Research Paper Topicsgihodatodev2100% (1)
- Strengthening The Rights of People With Psycho Social Disabilities in AfricaDocumento95 páginasStrengthening The Rights of People With Psycho Social Disabilities in AfricaAnnie Robb50% (4)
- Mha Discussion Paper 1 Introduction Key ComponentsDocumento5 páginasMha Discussion Paper 1 Introduction Key ComponentsDavid QatamadzeAinda não há avaliações
- National Mental Health ProgrammeDocumento36 páginasNational Mental Health ProgrammeSusmita Halder100% (1)
- Community Mental Health Services in Latin America For People With Severe Mental DisordersDocumento23 páginasCommunity Mental Health Services in Latin America For People With Severe Mental DisordersGloria ThomasAinda não há avaliações
- Mental Health ProgramDocumento4 páginasMental Health ProgramFernando GuyongAinda não há avaliações
- Satcher 2000 - Executive Summary - A Report of The SG On Mental HealthDocumento13 páginasSatcher 2000 - Executive Summary - A Report of The SG On Mental HealthSivaprakash BalasundaramAinda não há avaliações
- Ubwa 1Documento8 páginasUbwa 1simonAinda não há avaliações
- Geriatrics Elective2Documento5 páginasGeriatrics Elective2miibabhiekAinda não há avaliações
- Personality Disorders by DSM IVDocumento35 páginasPersonality Disorders by DSM IVJana ChihaiAinda não há avaliações
- Understanding and Avoiding The Nocebo EffectDocumento3 páginasUnderstanding and Avoiding The Nocebo EffectJana ChihaiAinda não há avaliações
- Final - Prevention of Coercion in Public Mental Health Care With Family Group ConferencingDocumento3 páginasFinal - Prevention of Coercion in Public Mental Health Care With Family Group ConferencingJana ChihaiAinda não há avaliações
- Clinical PsychologyDocumento54 páginasClinical PsychologyJana ChihaiAinda não há avaliações
- Katschnig TRIPS-2 - Interview English PDFDocumento12 páginasKatschnig TRIPS-2 - Interview English PDFJana ChihaiAinda não há avaliações
- Guidebook Evaluation Stigma Patrick CarriganDocumento66 páginasGuidebook Evaluation Stigma Patrick CarriganJana ChihaiAinda não há avaliações
- Panss PDFDocumento10 páginasPanss PDFJana Chihai50% (2)
- The Covid 19 Pandemic: Prepared By: Ken Jared P. MolatoDocumento6 páginasThe Covid 19 Pandemic: Prepared By: Ken Jared P. MolatoElvie Jane P. MolatoAinda não há avaliações
- Province of South Cotabato: Integrated SchoolsDocumento2 páginasProvince of South Cotabato: Integrated SchoolsDrwiAn DarAinda não há avaliações
- AcalasiaDocumento7 páginasAcalasiaEli JimenezAinda não há avaliações
- DOLE Labor Advisory 04 S. 2020Documento34 páginasDOLE Labor Advisory 04 S. 2020MyanAinda não há avaliações
- Food Safety PlanDocumento50 páginasFood Safety PlanCátia Costa0% (1)
- Opthalmology History Taking and Physical ExaminationsDocumento2 páginasOpthalmology History Taking and Physical ExaminationsZi Song100% (4)
- 13463-Article Text-25834-1-10-20210103Documento3 páginas13463-Article Text-25834-1-10-20210103Melly SyafridaAinda não há avaliações
- Clemente V GSISDocumento2 páginasClemente V GSISAnonymous wDganZAinda não há avaliações
- Morning Report Case Presentation: APRIL 1, 2019Documento14 páginasMorning Report Case Presentation: APRIL 1, 2019Emily EresumaAinda não há avaliações
- 2007 India CBSE Fact Sheet PDFDocumento2 páginas2007 India CBSE Fact Sheet PDFShanthi HariharanAinda não há avaliações
- Nonmalignant Leukocyte Disorder Chapter 26-35Documento15 páginasNonmalignant Leukocyte Disorder Chapter 26-35Reizel GaasAinda não há avaliações
- Neuromusculosklatal Disorders FK UnayaDocumento62 páginasNeuromusculosklatal Disorders FK UnayaSuci MayveraAinda não há avaliações
- Balancing Method MirroringDocumento9 páginasBalancing Method MirroringYoshua ViventiusAinda não há avaliações
- RandoxDocumento32 páginasRandoxIta MaghfirahAinda não há avaliações
- Plaster of ParisDocumento19 páginasPlaster of ParisayapillaiAinda não há avaliações
- By Richard Pinson, MD, FACP: Clinicians Often Struggle With The Distinction Between Delirium and EncephalopathyDocumento10 páginasBy Richard Pinson, MD, FACP: Clinicians Often Struggle With The Distinction Between Delirium and EncephalopathynoraAinda não há avaliações
- Eco506a Health Economics & Policy Problem SetDocumento13 páginasEco506a Health Economics & Policy Problem Setchandrakant kumarAinda não há avaliações
- DR D Kalpana, M.D, D.M (Neuro) Assoc. Professor of Pediatric Neurology, Medical College, TrivandrumDocumento54 páginasDR D Kalpana, M.D, D.M (Neuro) Assoc. Professor of Pediatric Neurology, Medical College, TrivandrumjspradeepscribdAinda não há avaliações
- Zika Virus - CDCDocumento5 páginasZika Virus - CDCLoretta McCalopeAinda não há avaliações
- A&P Principles of Microbiology and Human Disease (Nursing) - PowerPointDocumento47 páginasA&P Principles of Microbiology and Human Disease (Nursing) - PowerPointLinsey Bowen100% (2)
- The Watcher in The Shadows by Carlos Ruiz Zafon ExtractDocumento26 páginasThe Watcher in The Shadows by Carlos Ruiz Zafon ExtractOrion Publishing Group100% (1)
- National ExamDocumento55 páginasNational Examabel100% (1)
- CareMore: Innovative Healthcare DeliveryDocumento30 páginasCareMore: Innovative Healthcare DeliveryPartnership to Fight Chronic DiseaseAinda não há avaliações
- Mariko Aoki PhenomenonDocumento19 páginasMariko Aoki PhenomenonChristopher ServantAinda não há avaliações
- Alexithymia ArticleDocumento14 páginasAlexithymia ArticleDomingo MosqueraAinda não há avaliações
- Tinidazole Is An AntiDocumento6 páginasTinidazole Is An AntiNoi Maya Anggrita SariAinda não há avaliações
- IndianJOralSci5278-1137123 030931Documento5 páginasIndianJOralSci5278-1137123 030931Maqbul AlamAinda não há avaliações
- Key To Diagnosis in PaediatricsDocumento227 páginasKey To Diagnosis in PaediatricsVaishnavi SinghAinda não há avaliações
- CASE STUDIES L3 A Group 3Documento10 páginasCASE STUDIES L3 A Group 3Doneva Lyn MedinaAinda não há avaliações
- NursingWritingtests11 15Documento20 páginasNursingWritingtests11 15shiela8329gmailcom74% (27)