Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Curriculum de Hong-Kong - Ed. B - Sica-MatematicaDocumento292 páginasCurriculum de Hong-Kong - Ed. B - Sica-MatematicaGregório Silva NetoAinda não há avaliações
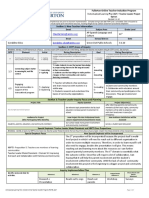
- Ilp FullertonDocumento3 páginasIlp Fullertonapi-467608657Ainda não há avaliações
- Muluken Alemayehu FINAL PDFDocumento47 páginasMuluken Alemayehu FINAL PDFKefi BelayAinda não há avaliações
- Plmun Thesis Mike MahorDocumento36 páginasPlmun Thesis Mike MahorPAUL DANIEL MAHORAinda não há avaliações
- Annals of Medicine and Surgery: Bliss J. ChangDocumento2 páginasAnnals of Medicine and Surgery: Bliss J. ChangroromutiaraAinda não há avaliações
- Rti 2Documento10 páginasRti 2REG.B/0620103018/LUQMAN AHMADAinda não há avaliações
- Perceived Benefits Received and Behavioral Intentions of Kabankalan Sinulog Festival TouristsDocumento14 páginasPerceived Benefits Received and Behavioral Intentions of Kabankalan Sinulog Festival TouristsMark GermanAinda não há avaliações
- Blood Drive ProposalDocumento4 páginasBlood Drive Proposalapi-250853393100% (2)
- HDFC Bank Project Saving AccountDocumento58 páginasHDFC Bank Project Saving Accountkunal srivastava100% (6)
- Step by Step Approach For Qualitative Data Analysis: Babatunde Femi AkinyodeDocumento12 páginasStep by Step Approach For Qualitative Data Analysis: Babatunde Femi AkinyodeSarras InfoAinda não há avaliações
- Adminstrative LawDocumento27 páginasAdminstrative LawGuru PrashannaAinda não há avaliações
- ACTION RESEARCH PRoposalDocumento2 páginasACTION RESEARCH PRoposalFritzAinda não há avaliações
- IELTS Vocabulary (1) JDocumento7 páginasIELTS Vocabulary (1) JBolorAinda não há avaliações
- ResumeDocumento1 páginaResumeapi-289204640Ainda não há avaliações
- O 1 Request PacketDocumento18 páginasO 1 Request PacketcdolekAinda não há avaliações
- UNICEF Childhood Disability in MalaysiaDocumento140 páginasUNICEF Childhood Disability in Malaysiaying reenAinda não há avaliações
- Unit 2: Data Collection and Sampling Techniques: Activating Prior KnowledgeDocumento12 páginasUnit 2: Data Collection and Sampling Techniques: Activating Prior KnowledgeMaricel ViloriaAinda não há avaliações
- (Cernea, 1995) Social Integration and Population DisplacementDocumento32 páginas(Cernea, 1995) Social Integration and Population DisplacementChica con cara de gatoAinda não há avaliações
- Module 2Documento6 páginasModule 2Christian DelfinAinda não há avaliações
- Shanthini InternDocumento25 páginasShanthini InternJayalakshmi RavichandranAinda não há avaliações
- Household Emergency Preparedness A Literature Review2012Journal of Community HealthDocumento9 páginasHousehold Emergency Preparedness A Literature Review2012Journal of Community HealthAyuAinda não há avaliações
- 1 Running Head: Nursing Theory AnalysisDocumento16 páginas1 Running Head: Nursing Theory AnalysisMa.Therese GarganianAinda não há avaliações
- NCM 116 SyllabusDocumento42 páginasNCM 116 SyllabusMiller Acompañado100% (8)
- Chanakya National Law University: Public International Law On The TopicDocumento4 páginasChanakya National Law University: Public International Law On The TopicKaran Singh RautelaAinda não há avaliações
- RRL DocumentDocumento16 páginasRRL DocumentTito CadeliñaAinda não há avaliações
- 提高创意写作的秘诀Documento13 páginas提高创意写作的秘诀afoddokhvhtldv100% (1)
- Summer Internship Project: ON Performance Appraisal Effectiveness IN Hindalco Flat Rolled Product, HirakudDocumento92 páginasSummer Internship Project: ON Performance Appraisal Effectiveness IN Hindalco Flat Rolled Product, HirakudUmrah NaushadAinda não há avaliações
- Mis CRMDocumento2 páginasMis CRMsolaiman93Ainda não há avaliações
- How To Write A Learning Contract PDFDocumento6 páginasHow To Write A Learning Contract PDFCustom Writing ServicesAinda não há avaliações
- 2014 15 GraduateDocumento306 páginas2014 15 GraduateyukmAinda não há avaliações