Você também pode gostar
- SJS Ten 1Documento10 páginasSJS Ten 1primatikaasAinda não há avaliações
- Background: Erythema MultiformeDocumento11 páginasBackground: Erythema MultiformeseidooreikiAinda não há avaliações
- Dress Syndrome With Mild Manifestations As A Diagnostic and Therapeutic Problem: Case ReportDocumento6 páginasDress Syndrome With Mild Manifestations As A Diagnostic and Therapeutic Problem: Case ReportEllya Latifah IlyasAinda não há avaliações
- Steven Johnson SyndromeDocumento13 páginasSteven Johnson SyndromeKhairul AnwarAinda não há avaliações
- Stevens Johnson DiseaseDocumento5 páginasStevens Johnson DiseaseShammy RNAinda não há avaliações
- Stevens-Johnson Syndrome: ClassificationDocumento3 páginasStevens-Johnson Syndrome: Classificationashvin_7Ainda não há avaliações
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDateDocumento41 páginasStevens-Johnson Syndrome and Toxic Epidermal Necrolysis - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDateDicky SangadjiAinda não há avaliações
- Causes, Pathophysiology, and Classification of Stevens-Johnson Syndrome (SJSDocumento23 páginasCauses, Pathophysiology, and Classification of Stevens-Johnson Syndrome (SJSrizqi_cepiAinda não há avaliações
- Rare Skin Disorder Stevens-Johnson SyndromeDocumento6 páginasRare Skin Disorder Stevens-Johnson SyndromeAudrey LeonarAinda não há avaliações
- ClinRevSJsyndrome PDFDocumento5 páginasClinRevSJsyndrome PDFMuhammad Nur Ardhi LahabuAinda não há avaliações
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFDocumento62 páginasStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFMatheus MeloAinda não há avaliações
- Journal Reading PersentationDocumento31 páginasJournal Reading PersentationKartikaEkaWulandariAinda não há avaliações
- Steven JohnsonDocumento36 páginasSteven JohnsonPrincess Louise ViceralAinda não há avaliações
- Drug Induced-Stevens Johnson Syndrome: A Case ReportDocumento26 páginasDrug Induced-Stevens Johnson Syndrome: A Case ReportdoktersandraAinda não há avaliações
- Stevens - Johnson SyndromeDocumento16 páginasStevens - Johnson SyndromeElvis obajeAinda não há avaliações
- Original Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearsDocumento6 páginasOriginal Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearssyalalaaalalaaaAinda não há avaliações
- Piis0002934310002937 PDFDocumento2 páginasPiis0002934310002937 PDFMuhammad TamlikhaAinda não há avaliações
- Stevens Johnson SyndromeDocumento14 páginasStevens Johnson SyndromeGaemkyulyea KVn100% (1)
- Retrospective Analysis of Deaths Due To Drug - Induced StevensJohnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) in Inpatients Admitted in The Dermatology Unit of A Tertiary Care HospitalDocumento4 páginasRetrospective Analysis of Deaths Due To Drug - Induced StevensJohnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) in Inpatients Admitted in The Dermatology Unit of A Tertiary Care HospitalIOSRjournalAinda não há avaliações
- Toxic Epidermal Necrolysis: BackgroundDocumento36 páginasToxic Epidermal Necrolysis: BackgroundGita AmeliaAinda não há avaliações
- Managing SJS: Diagnosis, Treatment and PreventionDocumento11 páginasManaging SJS: Diagnosis, Treatment and PreventionsyalalaaalalaaaAinda não há avaliações
- Anticonvulsant Hypersensitivity SyndromeDocumento8 páginasAnticonvulsant Hypersensitivity SyndromeMae Matira AbeladorAinda não há avaliações
- Adverse Cutaneous Drug Eruptions: Current Understanding: ReviewDocumento12 páginasAdverse Cutaneous Drug Eruptions: Current Understanding: ReviewasdasdAinda não há avaliações
- Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS) SyndromeDocumento7 páginasDrug Reaction With Eosinophilia and Systemic Symptoms (DRESS) SyndromeJeannette VillegasAinda não há avaliações
- Bullous Drug Reactions (Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) )Documento4 páginasBullous Drug Reactions (Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) )Putri ClaraAinda não há avaliações
- Drug Eruption: Li Xiao-HongDocumento57 páginasDrug Eruption: Li Xiao-Hongapi-19916399Ainda não há avaliações
- Review On Terminalia ChebulaDocumento2 páginasReview On Terminalia ChebulaAman SrivastavaAinda não há avaliações
- Recurrent Erythema Multiforme: A Dental Case Report: ReviewDocumento4 páginasRecurrent Erythema Multiforme: A Dental Case Report: Reviewjenn_1228Ainda não há avaliações
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis - ClinicalKeyDocumento21 páginasStevens-Johnson Syndrome and Toxic Epidermal Necrolysis - ClinicalKeyMasithaAinda não há avaliações
- Ijccm 25 575Documento5 páginasIjccm 25 575Nandha KumarAinda não há avaliações
- Toxic Epidermal Necrolysis and Stevens Johnson Syndrome: Our Current UnderstandingDocumento8 páginasToxic Epidermal Necrolysis and Stevens Johnson Syndrome: Our Current UnderstandingjoyfullAinda não há avaliações
- Applied Therapeutics Lec 8Documento18 páginasApplied Therapeutics Lec 8human.44697Ainda não há avaliações
- Evans Syndrome - StatPearls - NCBI BookshelfDocumento4 páginasEvans Syndrome - StatPearls - NCBI BookshelfJunbek nov23Ainda não há avaliações
- Anesthesia For Systemic Lupus Erythematosus ReviewDocumento12 páginasAnesthesia For Systemic Lupus Erythematosus ReviewAnonymous x75qV3lGAinda não há avaliações
- Wells Syndrome (Eosinophilic Cellulitis) : Proposed Diagnostic Criteria and A Literature Review of The Drug-Induced VariantDocumento8 páginasWells Syndrome (Eosinophilic Cellulitis) : Proposed Diagnostic Criteria and A Literature Review of The Drug-Induced VariantAnamaria IuoraşAinda não há avaliações
- SJS (Jurnal)Documento6 páginasSJS (Jurnal)FerryRoferdiAinda não há avaliações
- Toxic Epidermal Necrolysis and Stevens-Johnson Syndrome ReviewDocumento5 páginasToxic Epidermal Necrolysis and Stevens-Johnson Syndrome ReviewNantini GopalAinda não há avaliações
- Adverse Cutaneous Drug EruptioDocumento13 páginasAdverse Cutaneous Drug EruptioPeroquieAinda não há avaliações
- Etiology SJS: 2.1. Infectious CausesDocumento2 páginasEtiology SJS: 2.1. Infectious CausessellyhdelhiAinda não há avaliações
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A ReviewDocumento6 páginasStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A ReviewDede Rahman AgustianAinda não há avaliações
- Clinical Features, Diagnosis, and Treatment of Erythema Multiforme: A Review For The Practicing DermatologistDocumento14 páginasClinical Features, Diagnosis, and Treatment of Erythema Multiforme: A Review For The Practicing DermatologistBiljana CavdarovskaAinda não há avaliações
- SJS Treatment and SymptomsDocumento27 páginasSJS Treatment and SymptomsFitri wijayaAinda não há avaliações
- Manipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeDocumento56 páginasManipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeVaibhav KrishnaAinda não há avaliações
- Biomedicines 10 02105Documento16 páginasBiomedicines 10 02105Fatimah AssagafAinda não há avaliações
- Case Report: Amoxycillin and Clavulanic Acid Induced Stevens-Johnson Syndrome: A Case ReportDocumento4 páginasCase Report: Amoxycillin and Clavulanic Acid Induced Stevens-Johnson Syndrome: A Case ReportEkaAriawanAinda não há avaliações
- Erythema MultiformeDocumento22 páginasErythema MultiformeCoral Srinivasa RamaluAinda não há avaliações
- Number IV Erythema Multiforme: Mucosal Diseases SeriesDocumento7 páginasNumber IV Erythema Multiforme: Mucosal Diseases SeriesMely SalesAinda não há avaliações
- Pharmacology and therapeutics: Epidemiological and clinical features of severe adverse cutaneous drug eruptionsDocumento4 páginasPharmacology and therapeutics: Epidemiological and clinical features of severe adverse cutaneous drug eruptionsDee SobriAinda não há avaliações
- Ed Neutr 2022Documento32 páginasEd Neutr 2022Marga KouryAinda não há avaliações
- Inmuno NefritisDocumento6 páginasInmuno Nefritisjuan david castillo campoAinda não há avaliações
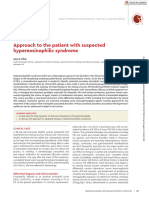
- Approach To Suspected Hypereosinophilic Syndrome ASHBloodDocumento8 páginasApproach To Suspected Hypereosinophilic Syndrome ASHBloodarimasen88Ainda não há avaliações
- Stevens-Johnson Syndrome: Review of The Literature: Stitt CarolinaDocumento4 páginasStevens-Johnson Syndrome: Review of The Literature: Stitt CarolinaNurul AfiahAinda não há avaliações
- Cutaneous Adverse Drug ReactionsDocumento5 páginasCutaneous Adverse Drug ReactionsEpi PanjaitanAinda não há avaliações
- 1 s2.0 S0738081X15001200 MainDocumento4 páginas1 s2.0 S0738081X15001200 MainPeem PrinAinda não há avaliações
- Systemic Lupus Erythematosus: Authors: DR Jessica J Manson and DR Anisur RahmanDocumento0 páginaSystemic Lupus Erythematosus: Authors: DR Jessica J Manson and DR Anisur RahmanRizka Norma WiwekaAinda não há avaliações
- Evans SyndromeDocumento13 páginasEvans SyndromerizeviAinda não há avaliações
- Putra,+18 Bmj.v5i1.274Documento9 páginasPutra,+18 Bmj.v5i1.274noor hidayahAinda não há avaliações
- Toxic Epidermal Necrolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandToxic Epidermal Necrolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Drug-Induced Oral ComplicationsNo EverandDrug-Induced Oral ComplicationsSarah CoustyAinda não há avaliações
- Fibromyalgia SyndromeNo EverandFibromyalgia SyndromeJacob N. AblinAinda não há avaliações
- KG For Issue For TheDocumento1 páginaKG For Issue For TheArief GusmanAinda não há avaliações
- Gaji Orng TuaDocumento1 páginaGaji Orng TuaArief GusmanAinda não há avaliações
- Title: 1. Heading 1Documento1 páginaTitle: 1. Heading 1JrRolandoAinda não há avaliações
- Lampiran Pengajaran Tindakan Medik IcuDocumento7 páginasLampiran Pengajaran Tindakan Medik IcuArief GusmanAinda não há avaliações
- Jsjaus Jsshsgsvs HDocumento1 páginaJsjaus Jsshsgsvs HArief GusmanAinda não há avaliações
- Teefd ShirtDocumento1 páginaTeefd ShirtArief GusmanAinda não há avaliações
- IfhehadbymyaDocumento1 páginaIfhehadbymyaArief GusmanAinda não há avaliações
- Ns Hihihi All DeeDocumento1 páginaNs Hihihi All DeeArief GusmanAinda não há avaliações
- Jdjjsas To Saayyy GotDocumento1 páginaJdjjsas To Saayyy GotArief GusmanAinda não há avaliações
- Cito Agree ItDocumento1 páginaCito Agree ItArief GusmanAinda não há avaliações
- Got So Far ExDocumento1 páginaGot So Far ExArief GusmanAinda não há avaliações
- DddjddnksDocumento1 páginaDddjddnksArief GusmanAinda não há avaliações
- HusbandDocumento1 páginaHusbandArief GusmanAinda não há avaliações
- Nice UsDocumento1 páginaNice UsArief GusmanAinda não há avaliações
- Japan NeDocumento1 páginaJapan NeArief GusmanAinda não há avaliações
- Hi Ben IsDocumento1 páginaHi Ben IsArief GusmanAinda não há avaliações
- Hi Ben IsDocumento1 páginaHi Ben IsArief GusmanAinda não há avaliações
- Jajiwhe Shhshs HahsahcfdfDocumento1 páginaJajiwhe Shhshs HahsahcfdfArief GusmanAinda não há avaliações
- SohedohesayDocumento1 páginaSohedohesayArief GusmanAinda não há avaliações
- DocumentDocumento1 páginaDocumentArief GusmanAinda não há avaliações
- Call LetterDocumento1 páginaCall LetterArief GusmanAinda não há avaliações
- My Had He SCHDocumento1 páginaMy Had He SCHArief GusmanAinda não há avaliações
- Jajiwhe Shhshs Hahsahcfdf ST GohfvDocumento1 páginaJajiwhe Shhshs Hahsahcfdf ST GohfvArief GusmanAinda não há avaliações
- But SheDocumento1 páginaBut SheArief GusmanAinda não há avaliações
- Jajiwhe Shhshs Hahsahcfdf ST GoDocumento1 páginaJajiwhe Shhshs Hahsahcfdf ST GoArief GusmanAinda não há avaliações
- Jajiwhe Shhshs HahsahDocumento1 páginaJajiwhe Shhshs HahsahArief GusmanAinda não há avaliações
- Xxyh GSSR HFDDocumento1 páginaXxyh GSSR HFDArief GusmanAinda não há avaliações
- Shjsgsgs HsjhssDocumento1 páginaShjsgsgs HsjhssArief GusmanAinda não há avaliações
- Do GHFFDocumento1 páginaDo GHFFArief GusmanAinda não há avaliações
- IfsoinDocumento1 páginaIfsoinArief GusmanAinda não há avaliações