Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- BIOCHEMISTRY BOARD EXAM QUESTIONS-answersDocumento7 páginasBIOCHEMISTRY BOARD EXAM QUESTIONS-answerschristinejoan100% (5)
- Genetics of RetinoblastomaDocumento5 páginasGenetics of RetinoblastomadesmawitaAinda não há avaliações
- Rat DissectionDocumento15 páginasRat Dissectionapi-233187566Ainda não há avaliações
- IchthyosisDocumento154 páginasIchthyosisprajnamitaAinda não há avaliações
- Basic Concepts of Genes, Chromosomes & DnaDocumento13 páginasBasic Concepts of Genes, Chromosomes & DnaAastha RamawatAinda não há avaliações
- Handbook of PhytoremediationDocumento840 páginasHandbook of Phytoremediationchoqollo100% (3)
- FRCRpart1BOF PDFDocumento36 páginasFRCRpart1BOF PDFlanka007100% (1)
- Gopu.R:::: Patient Age / Sex 30 Y / Male BranchDocumento1 páginaGopu.R:::: Patient Age / Sex 30 Y / Male BranchGopu RAinda não há avaliações
- 2011 Honda Insight Personalized Settings: Customer's NameDocumento2 páginas2011 Honda Insight Personalized Settings: Customer's Namelanka007Ainda não há avaliações
- Power Socket (1 Gang) : Instruction ManualDocumento23 páginasPower Socket (1 Gang) : Instruction Manuallanka007Ainda não há avaliações
- SLT Peo Router 2020 SettingsDocumento19 páginasSLT Peo Router 2020 Settingslanka007Ainda não há avaliações
- Kalana Maduwage: Identification of Venomous Snakes of Sri LankaDocumento2 páginasKalana Maduwage: Identification of Venomous Snakes of Sri Lankalanka007Ainda não há avaliações
- CA Bowel Follw UpDocumento1 páginaCA Bowel Follw Uplanka007Ainda não há avaliações
- Chemo ExtravasationDocumento12 páginasChemo Extravasationlanka007Ainda não há avaliações
- Model Paper Government College University, FaisalabadDocumento4 páginasModel Paper Government College University, FaisalabadieshrliuthlAinda não há avaliações
- Andrographis Paniculata A Review ofDocumento12 páginasAndrographis Paniculata A Review oftio_bsAinda não há avaliações
- Module 13 Study Guide - Phylum ChordataDocumento6 páginasModule 13 Study Guide - Phylum Chordataapi-233817991Ainda não há avaliações
- Viral Genetics PDFDocumento37 páginasViral Genetics PDFTemu Pisah100% (1)
- Heberprot PDocumento5 páginasHeberprot PManzoor A. ShaikhAinda não há avaliações
- 07 10 2021 Bio AssignmentDocumento4 páginas07 10 2021 Bio AssignmentSuneel ReddyAinda não há avaliações
- Chapter 56 Conservation Biology and Restoration EcologyDocumento4 páginasChapter 56 Conservation Biology and Restoration EcologyAndyAinda não há avaliações
- Genetic Disorders Associated With MeiosisDocumento1 páginaGenetic Disorders Associated With MeiosisJayrelle D. SafranAinda não há avaliações
- Paper 3 Experiment No: 6Documento2 páginasPaper 3 Experiment No: 6Asha AlmeidaAinda não há avaliações
- Topics For Speech in ScienceDocumento3 páginasTopics For Speech in ScienceAbhishek PubbisettyAinda não há avaliações
- UPDATED Annotated Cell DiagramDocumento3 páginasUPDATED Annotated Cell DiagramJ pAinda não há avaliações
- The Theory of Evolution Throughout HistoryDocumento18 páginasThe Theory of Evolution Throughout HistoryTupu AdreAinda não há avaliações
- Mammalian Oocyte Regulation Methoda and ProtocolesDocumento316 páginasMammalian Oocyte Regulation Methoda and ProtocolesTlad AljazeraAinda não há avaliações
- Kuliah Umum TransfusiDocumento54 páginasKuliah Umum TransfusiAnton TriyadiAinda não há avaliações
- Review Article On BarbituratesDocumento32 páginasReview Article On BarbituratesChelsea Ritz MendozaAinda não há avaliações
- Anti Egfr in MCRCDocumento64 páginasAnti Egfr in MCRCHemanth KumarAinda não há avaliações
- Gel Electrophoresis Lesson PlanDocumento8 páginasGel Electrophoresis Lesson Planapi-215898557Ainda não há avaliações
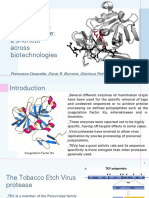
- Tobacco Etch Virus Protease: A Shortcut Across BiotechnologiesDocumento16 páginasTobacco Etch Virus Protease: A Shortcut Across BiotechnologiesNhật ThiệnAinda não há avaliações
- Animal Nutrition - CrosswordDocumento2 páginasAnimal Nutrition - CrosswordzeqialAinda não há avaliações
- b28113433 PDFDocumento202 páginasb28113433 PDFJuthika GogoiAinda não há avaliações
- Presentation1 171022084035Documento16 páginasPresentation1 171022084035Akkipero123Ainda não há avaliações
- Answer 1:: (Class - XII)Documento6 páginasAnswer 1:: (Class - XII)Subhadip MurmuAinda não há avaliações
- Colorectal Cancer A ReviewDocumento11 páginasColorectal Cancer A ReviewMarcelitaTaliaDuwiriAinda não há avaliações