Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Handbook5 PDFDocumento257 páginasHandbook5 PDFZAKROUNAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Virtual Work 3rd Year Structural EngineeringDocumento129 páginasVirtual Work 3rd Year Structural EngineeringStefano Martin PorciunculaAinda não há avaliações
- Centrifugal CastingDocumento266 páginasCentrifugal Castinguzairmetallurgist100% (2)
- Jet Bit Nozzle Size SelectionDocumento46 páginasJet Bit Nozzle Size SelectionBharat BhattaraiAinda não há avaliações
- Control System (136-248) PDFDocumento113 páginasControl System (136-248) PDFmuruganAinda não há avaliações
- Lightweight UavDocumento149 páginasLightweight Uavvb corpAinda não há avaliações
- Introduction To XAFSDocumento270 páginasIntroduction To XAFSEric William CochranAinda não há avaliações
- Thermal Analysis of Albendazole Investigated by HSM, DSC and FTIRDocumento8 páginasThermal Analysis of Albendazole Investigated by HSM, DSC and FTIRElvina iskandarAinda não há avaliações
- Orthodontic Extrusion of Premolar Teeth - An Improved TechniqueDocumento6 páginasOrthodontic Extrusion of Premolar Teeth - An Improved TechniquejorgeAinda não há avaliações
- Soft Tissues Remodeling Technique As A N PDFDocumento12 páginasSoft Tissues Remodeling Technique As A N PDFjorgeAinda não há avaliações
- Moraschini 2015Documento11 páginasMoraschini 2015jorgeAinda não há avaliações
- Effect of Abutment Tooth Color, Cement Color, and Ceramic Thickness On The Resulting Optical Color of A CAD: CAM Glass-Ceramic Lithium Disilicate - Reinforced Crown PDFDocumento8 páginasEffect of Abutment Tooth Color, Cement Color, and Ceramic Thickness On The Resulting Optical Color of A CAD: CAM Glass-Ceramic Lithium Disilicate - Reinforced Crown PDFjorgeAinda não há avaliações
- 7 Study of The Acceptability of Lateral Interocclusal Records by A Modular ArticulatorDocumento4 páginas7 Study of The Acceptability of Lateral Interocclusal Records by A Modular ArticulatorjorgeAinda não há avaliações
- Evaluation of The Marginal and Internal Discrepancies of CAD:CAM Endocrowns With Different Cavity Depths - An in Vitro StudyDocumento7 páginasEvaluation of The Marginal and Internal Discrepancies of CAD:CAM Endocrowns With Different Cavity Depths - An in Vitro StudyjorgeAinda não há avaliações
- Ahmed Et Al-2016-Journal of Esthetic and Restorative DentistryDocumento3 páginasAhmed Et Al-2016-Journal of Esthetic and Restorative DentistryAdrian YohanesAinda não há avaliações
- Grossmann2005 PDFDocumento4 páginasGrossmann2005 PDFjorgeAinda não há avaliações
- Imburgia DSD PosterDocumento1 páginaImburgia DSD PosterjorgeAinda não há avaliações
- BFEP2Documento6 páginasBFEP2jorgeAinda não há avaliações
- Gingival Zenith Positions and Levels of The MaxillaryDocumento9 páginasGingival Zenith Positions and Levels of The MaxillaryNia AlfaroAinda não há avaliações
- Bidra '13Documento18 páginasBidra '13jorgeAinda não há avaliações
- Experimental Birefringence Photography in DentistryDocumento12 páginasExperimental Birefringence Photography in Dentistryjorge100% (1)
- Dr. Mezmer's Psychopedia of Bad PsychologyDocumento378 páginasDr. Mezmer's Psychopedia of Bad PsychologyArt Marr100% (5)
- Modeling Mantle Convection CurrentsDocumento3 páginasModeling Mantle Convection Currentsapi-217451187Ainda não há avaliações
- Amateur's Telescope Was First Published in 1920. However, Unlike Ellison's TimeDocumento4 páginasAmateur's Telescope Was First Published in 1920. However, Unlike Ellison's Timemohamadazaresh0% (1)
- Lab Instruments GuideDocumento19 páginasLab Instruments GuideDesQuina DescoAinda não há avaliações
- Direct Determination of The Flow Curves of NoDocumento4 páginasDirect Determination of The Flow Curves of NoZaid HadiAinda não há avaliações
- Offshore Pipeline Hydraulic and Mechanical AnalysesDocumento25 páginasOffshore Pipeline Hydraulic and Mechanical AnalysesEslam RedaAinda não há avaliações
- Levee Drain Analysis in SlideDocumento12 páginasLevee Drain Analysis in SlideAdriRGAinda não há avaliações
- MechanicsDocumento558 páginasMechanicsfejiloAinda não há avaliações
- Hiad 2Documento15 páginasHiad 2Hrishikesh JoshiAinda não há avaliações
- Abaqus Analysis User's Manual, 32.15 (User Elements)Documento22 páginasAbaqus Analysis User's Manual, 32.15 (User Elements)Elias BuAinda não há avaliações
- NCHRP RPT 242 PDFDocumento85 páginasNCHRP RPT 242 PDFDavid Drolet TremblayAinda não há avaliações
- Mapua Institute of Technology: Field Work 1 Pacing On Level GroundDocumento7 páginasMapua Institute of Technology: Field Work 1 Pacing On Level GroundIan Ag-aDoctorAinda não há avaliações
- Electrostatic Discharge Ignition of Energetic MaterialsDocumento9 páginasElectrostatic Discharge Ignition of Energetic Materialspamos1111Ainda não há avaliações
- Electrical Conductivity of Carbon Blacks Under CompressionDocumento7 páginasElectrical Conductivity of Carbon Blacks Under CompressionМирослав Кузишин100% (1)
- JEE Class Companion Physics: Module-9Documento227 páginasJEE Class Companion Physics: Module-9RupakAinda não há avaliações
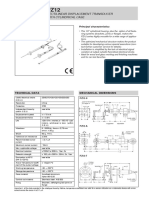
- Rectilinear Displacement Transducer With Cylindrical Case: Technical Data Mechanical DimensionsDocumento2 páginasRectilinear Displacement Transducer With Cylindrical Case: Technical Data Mechanical Dimensionsl561926Ainda não há avaliações
- Cara SamplingDocumento8 páginasCara SamplingAngga Dwi PutrantoAinda não há avaliações
- Design Steel Compression MembersDocumento42 páginasDesign Steel Compression MembersFayyazAhmadAinda não há avaliações
- M.Prasad Naidu MSC Medical Biochemistry, PH.D Research ScholarDocumento31 páginasM.Prasad Naidu MSC Medical Biochemistry, PH.D Research ScholarDr. M. Prasad NaiduAinda não há avaliações
- Name: Teacher: Date: Score:: Identify The Properties of MathematicsDocumento2 páginasName: Teacher: Date: Score:: Identify The Properties of MathematicsMacPapitaAinda não há avaliações
- Modeling Arterial Blood Flow With Navier-StokesDocumento15 páginasModeling Arterial Blood Flow With Navier-Stokesapi-358127907100% (1)
- Renewableand Sustainable Energy ReviewsDocumento9 páginasRenewableand Sustainable Energy Reviewssundeep sAinda não há avaliações