Você também pode gostar
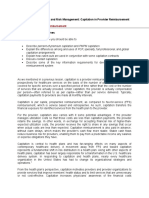
- Chapter 6 - Capitation in Provider ReimbursementDocumento23 páginasChapter 6 - Capitation in Provider ReimbursementAdityaAinda não há avaliações
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersAinda não há avaliações
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordNo EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordAinda não há avaliações
- AHM 250 4 Provider CompensationDocumento16 páginasAHM 250 4 Provider Compensationdeepakraj610Ainda não há avaliações
- Chapter 2 - Types of RiskDocumento20 páginasChapter 2 - Types of RiskAdityaAinda não há avaliações
- Healthcare Domain KnowledgeDocumento5 páginasHealthcare Domain KnowledgeRaghu TejaAinda não há avaliações
- A few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentNo EverandA few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentAinda não há avaliações
- Utilization Review Coordinator: Passbooks Study GuideNo EverandUtilization Review Coordinator: Passbooks Study GuideAinda não há avaliações
- HSMN Healthcare Payment MethodologiesDocumento20 páginasHSMN Healthcare Payment MethodologiesMarvin Whitfield100% (1)
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsAinda não há avaliações
- Data-Driven Healthcare: Revolutionizing Patient Care with Data ScienceNo EverandData-Driven Healthcare: Revolutionizing Patient Care with Data ScienceAinda não há avaliações
- The Healthcare Law and Ethics: Principles & PracticesNo EverandThe Healthcare Law and Ethics: Principles & PracticesAinda não há avaliações
- Cost, Payment and Proft AnalysisDocumento5 páginasCost, Payment and Proft Analysisbrodgerw_528691660Ainda não há avaliações
- Medicaid Claims Examiner: Passbooks Study GuideNo EverandMedicaid Claims Examiner: Passbooks Study GuideAinda não há avaliações
- Whose Patient Is ItDocumento3 páginasWhose Patient Is ItSean RAinda não há avaliações
- Supervising Registered Nurse: Passbooks Study GuideNo EverandSupervising Registered Nurse: Passbooks Study GuideAinda não há avaliações
- Health Record Technician I: Passbooks Study GuideNo EverandHealth Record Technician I: Passbooks Study GuideAinda não há avaliações
- Healthcare Environmental Services A Complete Guide - 2020 EditionNo EverandHealthcare Environmental Services A Complete Guide - 2020 EditionAinda não há avaliações
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipAinda não há avaliações
- Revenue Cycle Management A Complete Guide - 2019 EditionNo EverandRevenue Cycle Management A Complete Guide - 2019 EditionAinda não há avaliações
- The Protection of Employee Entitlements in Insolvency: An Australian PerspectiveNo EverandThe Protection of Employee Entitlements in Insolvency: An Australian PerspectiveAinda não há avaliações
- Pharmaceutical Care Services Guidelines DD v1!2!15 Apr 2019 2Documento37 páginasPharmaceutical Care Services Guidelines DD v1!2!15 Apr 2019 2Dinesh Kumar YadavAinda não há avaliações
- Health Informatics Service Architecture A Complete Guide - 2021 EditionNo EverandHealth Informatics Service Architecture A Complete Guide - 2021 EditionAinda não há avaliações
- Healthcare Payer Transformation A Complete Guide - 2019 EditionNo EverandHealthcare Payer Transformation A Complete Guide - 2019 EditionAinda não há avaliações
- Provider Revenue Cycle Management A Complete Guide - 2020 EditionNo EverandProvider Revenue Cycle Management A Complete Guide - 2020 EditionAinda não há avaliações
- Provider-Led Population Health Management: Key Strategies for Healthcare in the Cognitive EraNo EverandProvider-Led Population Health Management: Key Strategies for Healthcare in the Cognitive EraAinda não há avaliações
- Electronic Health Records: An Audit and Internal Control GuideNo EverandElectronic Health Records: An Audit and Internal Control GuideAinda não há avaliações
- Employment Consultant (Testing): Passbooks Study GuideNo EverandEmployment Consultant (Testing): Passbooks Study GuideAinda não há avaliações
- Medical equipment management Complete Self-Assessment GuideNo EverandMedical equipment management Complete Self-Assessment GuideAinda não há avaliações
- Modern Healthcare: How Can Digital Tools Help Improve Our Overall HealthNo EverandModern Healthcare: How Can Digital Tools Help Improve Our Overall HealthAinda não há avaliações
- Models of Care Delivery in NursingDocumento16 páginasModels of Care Delivery in NursingWalid Gee AbdulrahimAinda não há avaliações
- Healthcare Master Data A Complete Guide - 2020 EditionNo EverandHealthcare Master Data A Complete Guide - 2020 EditionAinda não há avaliações
- The Law of Healthcare Administration, Tenth EditionNo EverandThe Law of Healthcare Administration, Tenth EditionAinda não há avaliações
- Health Information Technology A Complete Guide - 2020 EditionNo EverandHealth Information Technology A Complete Guide - 2020 EditionAinda não há avaliações
- Guide to Healthcare Information Protection and Privacy for ExecutivesNo EverandGuide to Healthcare Information Protection and Privacy for ExecutivesAinda não há avaliações
- Healthcare Delivery Organization CIOs A Complete Guide - 2019 EditionNo EverandHealthcare Delivery Organization CIOs A Complete Guide - 2019 EditionAinda não há avaliações
- Textbook of Urgent Care Management: Chapter 7, Exit Transactions: The Process of Selling an Urgent Care CenterNo EverandTextbook of Urgent Care Management: Chapter 7, Exit Transactions: The Process of Selling an Urgent Care CenterAinda não há avaliações
- Textbook of Urgent Care Management: Chapter 9, Insurance Requirements for the Urgent Care CenterNo EverandTextbook of Urgent Care Management: Chapter 9, Insurance Requirements for the Urgent Care CenterAinda não há avaliações
- Ahima Data Quality Management ModelDocumento11 páginasAhima Data Quality Management Modelselinasimpson2301Ainda não há avaliações
- Textbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesNo EverandTextbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesAinda não há avaliações
- Purchasing Medical Innovation: The Right Technology, for the Right Patient, at the Right PriceNo EverandPurchasing Medical Innovation: The Right Technology, for the Right Patient, at the Right PriceAinda não há avaliações
- Measuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsNo EverandMeasuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsAinda não há avaliações
- Scaling Up Inclusive Healthcare Initiatives in Lmic ForwebDocumento30 páginasScaling Up Inclusive Healthcare Initiatives in Lmic ForwebIgor IlievskiAinda não há avaliações
- The Citizen Patient: Reforming Health Care for the Sake of the Patient, Not the SystemNo EverandThe Citizen Patient: Reforming Health Care for the Sake of the Patient, Not the SystemAinda não há avaliações
- Care ManualDocumento70 páginasCare ManualQMx2014Ainda não há avaliações
- Testimonialsand FeedbackDocumento1 páginaTestimonialsand FeedbackAdityaAinda não há avaliações
- Module 6Documento4 páginasModule 6AdityaAinda não há avaliações
- Trait Chart and Handwriting SampleDocumento5 páginasTrait Chart and Handwriting SampleAdityaAinda não há avaliações
- Detailed Analysis PDFDocumento6 páginasDetailed Analysis PDFAdityaAinda não há avaliações
- RecipesDocumento14 páginasRecipesAdityaAinda não há avaliações
- Sample AnalysisDocumento3 páginasSample AnalysisAdityaAinda não há avaliações
- Vocational AnalysisDocumento4 páginasVocational AnalysisAdityaAinda não há avaliações
- Testimonialsand FeedbackDocumento1 páginaTestimonialsand FeedbackAdityaAinda não há avaliações
- NewDocumento14 páginasNewAdityaAinda não há avaliações
- Detailed AnalysisDocumento6 páginasDetailed AnalysisAditya100% (1)
- L2 Final HW SpecimensDocumento1 páginaL2 Final HW SpecimensAdityaAinda não há avaliações
- Assignment Module1to5Documento14 páginasAssignment Module1to5AdityaAinda não há avaliações
- Handwriting Analysts International: Level 2 Proficiency ExamDocumento1 páginaHandwriting Analysts International: Level 2 Proficiency ExamAdityaAinda não há avaliações
- Compatibility Report For M. and L.: Grapho Logy Is The Scientific Examination of A Person's HandwritingDocumento4 páginasCompatibility Report For M. and L.: Grapho Logy Is The Scientific Examination of A Person's HandwritingAdityaAinda não há avaliações
- Handwriting rhythm traitsDocumento5 páginasHandwriting rhythm traitsAdityaAinda não há avaliações
- Cover PageDocumento2 páginasCover PageAdityaAinda não há avaliações
- Ahm250 l19 PDFDocumento14 páginasAhm250 l19 PDFVinayaka KumarAinda não há avaliações
- Study on Budgetary Control at BPLDocumento3 páginasStudy on Budgetary Control at BPLAdityaAinda não há avaliações
- PSMDocumento1 páginaPSMAditya0% (1)
- Handwriting Analysts InternationalDocumento12 páginasHandwriting Analysts InternationalAdityaAinda não há avaliações
- Garmn Order DetailsDocumento1 páginaGarmn Order DetailsAdityaAinda não há avaliações
- Scrum Process Control EmpiricalDocumento17 páginasScrum Process Control EmpiricalAdityaAinda não há avaliações
- NexusGuide v1.1Documento11 páginasNexusGuide v1.1TITAITOQQAinda não há avaliações
- AHM 520: Provider Reimbursement and Plan RiskDocumento11 páginasAHM 520: Provider Reimbursement and Plan RiskRahul KoulAinda não há avaliações
- Chapter 3 - Risk Management in Health PlansDocumento19 páginasChapter 3 - Risk Management in Health PlansAdityaAinda não há avaliações
- Chapter 1 - Health Plan Financial InformationDocumento13 páginasChapter 1 - Health Plan Financial InformationAdityaAinda não há avaliações
- Revenue Cycle Management or Practice ManagementDocumento2 páginasRevenue Cycle Management or Practice Managementapi-76860857Ainda não há avaliações
- Case Study Ch. 3Documento4 páginasCase Study Ch. 3Rafania KinasihAinda não há avaliações
- Done For You Workouts For Tennis Ball Biceps and Horseshoe TricepsworkDocumento21 páginasDone For You Workouts For Tennis Ball Biceps and Horseshoe TricepsworkAndreJ.Rod100% (12)
- Sarocam Vs Interorient Maritime 493 Scra 502Documento19 páginasSarocam Vs Interorient Maritime 493 Scra 502lehsem20006985Ainda não há avaliações
- Health Insurance in KsaDocumento9 páginasHealth Insurance in KsaserlinaAinda não há avaliações
- Mission Health-HCA Healthcare Inc. Asset Purchase Agreement, Aug. 30, 2018Documento147 páginasMission Health-HCA Healthcare Inc. Asset Purchase Agreement, Aug. 30, 2018Dillon DavisAinda não há avaliações
- Meet The LMC's New PM RepresentativeDocumento8 páginasMeet The LMC's New PM RepresentativeCornwall and Isles of Scilly LMCAinda não há avaliações
- Swedish Medical Association Lakarforbundet Utomnordisk Examen EngDocumento7 páginasSwedish Medical Association Lakarforbundet Utomnordisk Examen Engbama6592Ainda não há avaliações
- LEGAL MEDICINE Midterms ReviewerDocumento2 páginasLEGAL MEDICINE Midterms ReviewerJames Gregory A. VillasisAinda não há avaliações
- Living WillDocumento4 páginasLiving Willchuckie72Ainda não há avaliações
- EnCORE v12-3 en EnglishDocumento134 páginasEnCORE v12-3 en EnglishGhulam MurtazaAinda não há avaliações
- Medical Claim Reimbursement Form EnglishDocumento2 páginasMedical Claim Reimbursement Form EnglishHananAhmedAinda não há avaliações
- Wisp Pediatric INTL OISDocumento182 páginasWisp Pediatric INTL OISAitorAinda não há avaliações
- Questionnaire work-life balanceDocumento5 páginasQuestionnaire work-life balancePurnima PuriAinda não há avaliações
- Pre Employment Joining ChecklistDocumento1 páginaPre Employment Joining ChecklistKunal SinghAinda não há avaliações
- Case Study-Misrepresentation by Life InsuredDocumento3 páginasCase Study-Misrepresentation by Life InsuredFreddy Savio D'souzaAinda não há avaliações
- HHS OIG - Offshore Outsourcing OEI-09-12-00530Documento13 páginasHHS OIG - Offshore Outsourcing OEI-09-12-00530Michael BarbereAinda não há avaliações
- HMO NHIS GuidelinesDocumento18 páginasHMO NHIS Guidelinestitooluwa100% (1)
- Trinity Health v. Anesthesia Associates of Ann ArborDocumento53 páginasTrinity Health v. Anesthesia Associates of Ann ArborAlex KacikAinda não há avaliações
- SAMPLE Referral Management PolicyDocumento3 páginasSAMPLE Referral Management PolicyDarren Cariño100% (3)
- ContarctDocumento3 páginasContarctJunaid AnwerAinda não há avaliações
- Malpractice Proposal-Aijaz-NewDocumento2 páginasMalpractice Proposal-Aijaz-NewGalaleldin AliAinda não há avaliações
- Proving Medical Value Under HowellDocumento48 páginasProving Medical Value Under HowellJohn HentschelAinda não há avaliações
- Prelimin ImpressionsDocumento54 páginasPrelimin ImpressionsHamdallah FatayerAinda não há avaliações
- Pasay City General Hospital - LocationDocumento2 páginasPasay City General Hospital - LocationjrbautistaAinda não há avaliações
- Medical Devices Industry in IndiaDocumento39 páginasMedical Devices Industry in IndiaAnurag Rawat100% (2)
- Jimmy Steel ReportDocumento86 páginasJimmy Steel ReportemmyvigoAinda não há avaliações
- Sim Vivo SutureDocumento12 páginasSim Vivo SutureYasser AhmedAinda não há avaliações
- General Requirements for Safe Blasting OperationsDocumento20 páginasGeneral Requirements for Safe Blasting Operationsz77ia100% (2)
- Work B.C.-letter of IntentDocumento2 páginasWork B.C.-letter of IntentValerie PetersAinda não há avaliações